

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Persistent infection with oncogenic human papillomavirus (HPV) types has been shown to be necessary for the development of cervical intraepithelial neoplasia (CIN 1) and cervical cancer. Therefore, testing for oncogenic HPV infection could serve as an accurate means of detecting women at risk for cervical cancer. Moreover, HPV testing would be required as a primary screening tool in the era of HPV vaccination [1]. Numerous studies have established that HPV DNA testing is significantly more sensitive than Pap cytology for the detection of high-grade cervical intraepithelial neoplasia (CIN 2) or worse, and it is recommended for primary cervical cancer screening and triage of borderline cytological abnormalities [2].
Since the 1960s, cytology-based screening has led to major reductions in the incidence of cervical cancer and related mortality. Due to the increased sensitivity of HPV DNA testing, the combined use of cytological testing and HPV DNA testing with Hybrid Capture 2 (HC2) (Qiagen, Gaithersburg, MD, USA) in screening has been approved by the US Food and Drug Administration (FDA) for women aged 30 yr and over. For the last decade, the HC2 test has been the most important HPV diagnostic assay, and it is still the most frequently used worldwide. In the last several years, advances in HPV detection methods have been made, and a wide variety of assays are now available [3]. The recently developed Abbott RealTime High Risk HPV PCR assay is a real-time PCR assay designed to detect not only 14 high-risk HPV genotypes, but also to simultaneously distinguish HPV type 16/18 from other HPV types. The application of this assay has yet to be investigated in Korea. LG Life Sciences (Seoul, Korea) has also developed a real-time PCR assay (AdvanSure HPV Screening real-time PCR), which detects not only 41 HPV genotypes, but also simultaneously differentiates HPV type 16/18 from other HPV types; however, the performance of this assay has yet to be investigated.
We evaluated the performance of the AdvanSure HPV Screening real-time PCR assay and the Abbott RealTime High Risk HPV PCR assay in comparison with the HC2 test using 177 liquid-based cytology samples for their ability to detect HPVs.
METHODS
1. Specimens
A total of 177 cytology specimens were obtained from women who visited the gynecology clinic at Ewha Womans University Mokdong Hospital from July to September 2010. The median age of the patients was 42 yr (range, 21-77). Pathological diagnoses on the basis of cervical cytology and Pap smear results were within the normal limits in 127 patients (72%). Atypical squamous cells of undetermined significance (ASC-US) were observed in 11 (7%), CIN1 in 19 (10%), CIN2 in 7 (4%), CIN3 in 9 (5%), and invasive carcinoma in 4 patients (2%). A single cervical specimen was collected from all participants using a cytobrush and was suspended into Cervical Sampler solution (Qiagen) according to the manufacturer's instructions.
2. Study design
All specimens were tested using the HC2, AdvanSure PCR, and Abbott PCR assays, and samples showing any discordant results were genotyped using INNO-LiPA HPV Genotyping (Innogenetics, Gent, Belgium) and/or sequencing. The samples that were negative in all 3 tests were considered negative in the consensus HPV result, and samples that were positive in all 3 tests were considered positive in the consensus HPV result. Other samples (N=37) with discrepant results in the 3 assays were typed by INNO-LiPA genotyping (N=34) and/or sequencing (N=11), and the consensus HPV result was determined based on the targeted HPV type [4]. For the consensus HPV result of any discrepant INNO-LiPA and sequencing results, either the INNO-LiPA or sequencing results were used. We calculated the sensitivity and specificity of each test based on the consensus HPV result. Additionally, in the 2 real-time PCR assays (AdvanSure PCR and Abbott PCR), the results for the detection of HPV 16/18 were also compared.
This study was approved by the institutional review boards of our institution.
3. Hybrid Capture 2 HPV DNA Test (HC2)
The Hybrid Capture 2 HPV DNA Test (Qiagen) is a sandwich capture molecular hybridization assay that provides a semi-quantitative result through chemiluminescent detection. This test can detect 13 high-risk (HR) HPV genotypes (HR: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68). This test was performed according to the manufacturer's instructions. Specimens with relative light unit/cutoff ratios (RLU/CO) ≥1.0 were considered positive.
4. AdvanSure HPV Screening real-time PCR assay (AdvanSure PCR)
The AdvanSure HPV Screening real-time PCR assay (LG Life Sciences) is a real-time PCR assay that detects 41 HPV genotypes (HR: 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 67, 68, 69, 70, 72, and 73; and low risk (LR): 3, 6, 10, 11, 27, 32, 34, 40, 42, 43, 44, 54, 55, 57, 61, 62, 71, 74, 81, and 84), and also differentiates HPV type 16/18 from other HPV types. In a single reaction, this test can detect and distinguish the signals for HPV 16/18 from non-16/18 types as well as an internal control. The test was performed according to the manufacturer's instructions.
5. Abbott RealTime High Risk HPV assay (Abbott PCR)
The Abbott RealTime High Risk HPV assay (Abbott Molecular, Abbott Park, IL, USA) is a real-time PCR assay developed for the detection of DNA from 14 high-risk HPV genotypes (HR: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68). HPV 16- and HPV 18-specific probes and a probe for human beta-globin (internal control) are labeled with different dyes while the other HR HPV probes are labeled with the same dye. The test was performed according to the manufacturer's instructions.
6. INNO-LiPA HPV Genotyping (INNO-LiPA)
The INNO-LiPA HPV Genotyping test (Innogenetics) is a genotyping assay based on reverse line-blot hybridization. This test allows for the identification of 28 HPV types (HR: 16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 69/71, 70, and 73; and LR: 6, 11, 34, 40, 42, 43, 44, 54, and 74). Testing was performed according to the manufacturer's instructions.
7. Sequencing
Two primers (MY and GP) were designed using internal fragments of the HPV L1 region (LG Life Sciences, Korea). PCR was performed using 10 µL of HS Taq premix (Genet Bio, Korea), 10 µL of each primer set and 10 µL of extracted template DNA in the Takara PCR Thermal Cycler Dice (Takara Bio INC., Japan). The PCR mixture was denatured for 5 min at 95℃, which was followed by 40 cycles of 15 sec at 95℃, 45 sec at 55℃, and 30 sec at 74℃ for the MY region, or 15 sec at 95℃, 45 sec at 48℃, and 30 sec at 74℃ for the GP region to amplify the PCR mixture. A final extension step was done at 72℃ for 5 min. The PCR products were purified using the QIAquick PCR purification kit (Qiagen, Germany). Sequencing of positive PCR samples was performed by Cosmogenetech Laboratory (Korea), and the DNA sequences were aligned with the basic local alignment search tool (BLAST) for analysis.
RESULTS
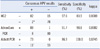
The sensitivities and specificities of the HC2, AdvanSure PCR, and Abbott PCR assays are shown in Table 1. We determined the consensus HPV result considering the target HPVs of each test and, in discrepant samples, the results of INNO-LiPA and/or sequencing. Additionally, we evaluated the accuracy of each test according to the consensus HPV result. The sensitivities of HC2, AdvanSure PCR, and Abbott PCR were 97.6%, 91.7%, and 86.9%, respectively, and the specificities were 83.9%, 98.8%, and 100.0%, respectively. The kappa coefficient between the consensus HPV result and HC2, AdvanSure PCR, and Abbott PCR were 0.8088, 0.8982, and 0.8745, respectively.
The discordant results in the HC2, AdvanSure PCR, and Abbott PCR assays are summarized in Table 2. Of the 177 samples, 140 (79%) showed concordant results in all 3 tests; 75 samples were positive in all 3 tests, and 65 were negative in all 3 tests. The remaining 37 samples showed discrepant results among the 3 tests. They were subsequently genotyped with INNO-LiPA (N=34) and/or sequencing (N=11).
According to the HPV types determined by INNO-LiPA and/or sequencing, the HC2 assay yielded 15 false-positive and 2 false-negative results, including 1 false-negative for HPV type 16. The AdvanSure PCR assay yielded 1 false-positive and 8 false-negative results, which included HPV types 51, 52, and 56. The Abbott PCR assay yielded only 11 false-negative results for samples containing HPV types 16, 31, 52, 56, 59, and 70, including 3 false-negative HPV type 16 samples.
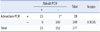
The 2 real-time PCR assays could separately detect oncogenic, HR HPV types 16 and/or 18; therefore, performance for the detection of HPV type 16 and/or 18 was compared for these 2 assays. Of the 177 samples, 25 samples were AdvanSure PCR (+)/Abbott PCR (+), 149 samples were AdvanSure PCR (-)/Abbott PCR (-), and 3 samples were AdvanSure PCR (+)/Abbott PCR (-). The concordance rate was 98.3%, and the kappa coefficient was 0.9335, which indicated nearly perfect concordance. Among the 3 discrepant samples, 1 sample was not only negative for types other than 16/18 (type 31, 52, and 70) but also negative for type 16, and the other 2 samples were positive for types other than 16/18 (type 52, 56, and 59), but negative for type 16 (Table 3).
DISCUSSION
The HC2 test has demonstrated the clinical value of HPV testing in most key randomized controlled clinical trials and other clinical trials [5-7]. Recently, it has been recommended that new HPV assays show clinical characteristics similar to the HC2 assay in the process of clinical validation of high risk-HPV tests before they can be used for cervical cancer screening purposes [2]. We investigated 2 real-time PCR assays (AdvanSure PCR and Abbott PCR) for HPV detection and compared them with the HC2 assay. We determined the consensus HPV result based on the results of the 3 assays and further genotyping assays for discrepant samples [4]. The performance of each assay was then compared with the consensus HPV result. In general, the evaluation of new tests consists of analytical and clinical performance (sensitivity, specificity, and detection limit), and a comparison between the new tests and a reference test; however, this study was limited to information comparing the 3 tests. Therefore, further studies are needed.
In the HC2 assay, the sensitivity was 97.6%, which was higher than that of the 2 real-time PCR assays (91.7% and 86.9%). However, 15 samples showed false-positive results, with a specificity of 83.9%, which was lower than the other 2 assays. The false-positive rate has been reported as 5.6-10.3% [8, 9]. This analytical inaccuracy has been suggested to be due to the cross-reactivity of the probe cocktail with untargeted HPV types [8-10]. A next-generation diagnostic system could resolve these problems [11].
The recently developed AdvanSure PCR assay is a real-time PCR assay designed to detect numerous HPV types (21 HR HPV types and 20 LR HPV types) and separately discriminate HPV types 16 and/or 18 from other types using an additional probe. With the AdvanSure PCR assay, 8.3% of samples (8/96) were false negatives, for a sensitivity of 91.7%, which was lower than that of the HC2 assay. These samples were genotyped using INNO-LiPA and/or sequencing as HPV types 51, 52, and 56. According to the AdvanSure PCR manual, the analytical sensitivities for these HPV types (10,000-100,000 copies/reaction) were relatively lower than that for the other types (1-1,000 copies/reaction) [12]. The specificity of the AdvanSure PCR assay was 98.8% and was higher than that of the HC2 assay. The kappa coefficient was almost perfect in the 3 tests, but that of the AdvanSure PCR assay (k=0.8982) was higher than that of the other 2 tests (0.8088 and 0.8745 for the HC2 and Abbott PCR assays, respectively). Although the AdvanSure PCR assay can detect most HPV types, it does not differentiate LR HPV from HR HPV, and the LR HPV types are too vague to suggest sufficient information to clinicians.
The Abbott PCR assay is also a real-time PCR assay based on concurrent individual genotyping for type 16 and/or type 18 and pooled detection of 12 other HR HPVs. In the Abbott PCR assay, no samples were false positive, so its specificity (100%) was the highest among the 3 assays. However, the sensitivity was 86.9%, the lowest among the 3 assays. We genotyped the false-negative samples (n=11), which contained HPV types 16, 51, 52, 56, and 59, and in 3 of the 11 false-negative samples, the clinically important HR HPV type 16 was not detected. According to previous studies [13-15], the agreements between the Abbott PCR assay and the HC2 assay, which has been FDA-approved to show scientific reproducibility, were approximately 93-95%. This false negativity may be due to low viral load and multiple infections. There were multiple infections (16, 31, 52, 56, 59, and 70) in 3 of the false negative samples where the Abbott PCR was positive for other HPVs and negative for HPV 16. According to the Abbott PCR assay manual, the analytical sensitivity for these HPV types was 500-2,000 copies/reaction [16]; however, we could not determine the viral load of these samples. The 2 real time PCR assays utilize a fully automated or semi-automated platform, so those assays are easier to perform than the HC2 assay.
In conclusion, the recently developed AdvanSure PCR and Abbott PCR assays are less sensitive than the HC2 assay, but more specific than the HC2 assay for the detection of HPV. The overall performance of the 2 real-time PCR assays is comparable to the HC2 assay, and these PCR assays can simultaneously differentiate HPV types 16/18 from other HPV types.

 XML Download
XML Download