

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Febrile seizure is one of the most common neurological problems during childhood [1]. Approximately 2-5% of children are estimated to experience at least 1 epileptic seizure during a febrile illness before they are 5 yr old. The incidence of febrile seizures varies between 2% and 4% in Western countries, whereas the incidence is 7% in Japan and higher in developing countries [2-4].
Febrile seizures occur during infancy or childhood, typically between 3 months to 5 yr of age. Seizures occurring with fever in children who have suffered a previous non-febrile seizure are excluded from the definition of febrile seizures. Febrile seizures should also be distinguished from epilepsy, which is characterized by recurrent non-febrile seizures [5].
The etiology and pathogenesis of febrile seizure remain unknown. However, several factors such as vitamin B6 deficiency, electrolyte disturbances, reduction in serum and cerebrospinal fluid (CSF) zinc levels, and low gamma-aminobutyric acid (GABA) levels are thought to play a role in the pathogenesis of febrile seizure [6-10]. Among these factors, low zinc levels in both the CSF and serum have attracted interest, and studies on the correlation between low serum zinc levels and febrile seizures are being currently conducted.
We compared serum zinc levels in preschool children with febrile seizures and those with afebrile seizures using inductively coupled plasma mass spectrometry (ICP-MS).
METHODS
We enrolled 288 children who were admitted to the Department of Pediatrics at the Samsung Changwon Hospital between January 1, 2009 and February 28, 2011. Medical records were retrospectively reviewed following approval for the study by the hospital Institutional Review Board. To avoid probable confounding factors, only the specimen of the first episode was considered for a case of multiple seizure attacks in a child, and children older than 60 months were excluded.
Febrile seizures were defined as seizures accompanied with fever (≥38℃) without central nervous system (CNS) infection, while afebrile seizures were defined as seizures due to non-febrile illness. Serum specimens were acquired from the febrile seizure and afebrile seizure group within the first 2 hr after a seizure attack. The specimens were stored at -20℃ until analysis. Serum zinc levels were analyzed using an Agilent 7500ce ICP-MS (Agilent Technologies, Inc., Tokyo, Japan). In addition, the serum C-reactive protein (CRP) level in each patient was measured for comparing serum zinc levels after correcting for acute inflammatory protein.
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) 12.0 software (SPSS, Inc., Chicago, IL, USA) for Windows and Medcalc v11.2 (Mariakerke, Belgium). Statistical significance was estimated using independent t-tests and an analysis of covariance (ANCOVA) test. P values less than 0.05 were considered significant.
RESULTS
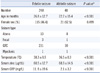
Characteristics of the patients included in this study are shown in Table 1. Mean temperatures of children in the febrile seizure and afebrile seizure groups were 38.3±0.9℃ and 36.5±0.3℃, respectively. Seizure was classified as atonic (N=21), focal (N=4), generalized tonic-clonic (N=261), or myoclonic (N=2).
Mean serum zinc levels in the febrile seizure and afebrile seizure groups were 60.5±12.7 µg/dL and 68.9±14.5 µg/dL, respectively. An independent t-test showed that the mean serum zinc levels in the febrile seizure group were significantly different (P<0.001) from those in the non-febrile seizure group. The difference was significant even after correcting for age using an ANCOVA test (P<0.001; Fig. 1).
Mean serum CRP levels in the febrile seizure and afebrile seizure groups were 11.8±19.6 mg/L and 2.1±3.2 mg/L, respectively; the intergroup difference in mean serum CRP levels was significant (P<0.001; Table 1). After correcting for serum CRP levels, the intergroup difference in the mean serum zinc levels was statstically significant (P=0.003).
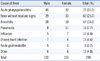
The most common cause of fever in the febrile seizure group was respiratory infections (62.5%) such as acute pharyngotonsillitis, bronchitis, pneumonia, and influenza (Table 2).
DISCUSSION
Zinc is one of the most abundant trace elements in the body and is found at a high level in the CNS where it influences cell division and differentiation, which are required for normal CNS development [11, 12]. Most of the zinc in the brain is bound to zinc-binding proteins that have functional and structural roles. A small portion of the zinc is present in the ion form; ionic zinc has been suggested to be involved in specific physiologic mechanisms including synaptic neurotransmission. The mechanism underlying the role of zinc levels in seizures has been examined in studies on mouse models and in vitro studies. A series of reports have suggested that zinc modulates specific GABA receptors, and this mechanism is known to contribute to seizure inhibition [13-15]. However, studies on humans have shown that the febrile seizure group has lower zinc level than the control group with simple fever, although there is some disagreement [16, 17].
In febrile seizure, hypozincemia has been suggested as a possible change during the rising phase of body temperature in patients. Fever is thought to be mediated by an endogenous pyrogen. The infection state exhibits a non-specific host responses, including immune responses such as changes in the concentrations of some plasma proteins. Many studies have shown that injecting infectious materials or cytokines such as tumor necrosis factor, interleukin-1, interleukin-6, and interferon causes hypozincemia accompanied by fever [18-23]. These results suggest that infection leads to hypozincemia through endogenous pyrogenic substances.
In our study, the febrile seizure group had significantly lower serum zinc levels than the afebrile group. We analyzed differences in serum zinc levels between the 2 groups after correcting for age and CRP levels and observed that the difference remained significant. Several reports have suggested that low serum levels of zinc may result in febrile seizures, but this is still debated. Gündüz et al. [24] compared serum and CSF zinc levels in patients with febrile and afebrile convulsions and healthy controls; they concluded that compared to patients with afebrile convulsions and healthy controls, patients with febrile convulsions had lower serum zinc levels. According to previous studies, compared to a control group with fever but no convulsions, children with febrile convulsions showed significantly lower serum zinc levels [6, 25].
In contrast to these previous studies, we analyzed data from a large number of children with febrile seizures and considered confounding factors such as age and CRP levels. Although the correlation between zinc levels and aging or acute phase status is still debatable, zinc levels are known to increase with age until adulthood, and the acute phase response has been associated with depressed serum zinc level in some studies [26, 27]. However, in our study, zinc levels were significantly different between the febrile and afebrile seizure groups after correcting for age or serum CRP levels.
We used ICP-MS, which is an effective technique for determining trace element levels [28-31]. Unlike inductively coupled plasma atomic emission spectrometry, ICP-MS can be used for direct analysis of solution samples, can be used to measure most elements, and provides much lower detection limits and reliable isotopic analysis [32].
One limitation of our study is the lack of a simple febrile or healthy control group. Furthermore, ICP-MS has been recently developed, and reference ranges for zinc levels have not yet been established. However, various analysis methods used in previous studies have shown that serum zinc levels in healthy children are higher than those in children with febrile seizure. Ganesh et al. reported that the mean serum zinc level as measured using atomic absorption spectrometry in samples from healthy children between 3 months and 5 yr of age was 87.6 µg/dL, and the corresponding value in children with simple febrile seizures was 32.17 µg/dL [16]. Another study using plasma emission spectrometry reported that serum zinc levels in patients with simple febrile seizure and acute febrile illness were 112.5 µg/dL and 154.1 µg/dL, respectively. A recent study of mean serum zinc levels in healthy adults using ICP-MS reported a similar result (80.45 µg/dL) [33]. Although the difference in the zinc levels in febrile seizure and afebrile seizure groups obtained in our study is smaller than that reported in previous studies, it is difficult to compare the serum zinc levels measured in the present study with those of the previous studies because the analysis methods used were different. However, on the basis of previous studies, serum zinc levels in healthy and simple fever groups were presumed to be higher than those in the febrile seizure group.
In this study, the serum zinc level in patients with febrile seizure and afebrile seizure groups showed large overlap. Serum zinc levels are influenced by the time of day, the specific disease, or the presence of other trace elements [34]. Therefore, a study design considering these effects is needed to further explain hypozincemia in febrile seizure children.
In conclusion, we showed that children with febrile seizures had significantly lower serum zinc levels than those with afebrile seizures. However, the mechanism of this altered serum zinc level in the febrile seizure group is poorly understood. Further studies are needed to identify the cause of this observation.

 XML Download
XML Download