

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
According to statistics, there were 438,000 live births in Korea in 2015, 52.3% of which were firstborns [1]. The rate of cesarean sections has steadily increased from 36% in in 2006 to 40.2% in 2015, and has shown a similar trend for nulliparous women, i.e., from 34.9% in 2006 to 42.3% in 2015 [2]. Supposing the absence of a previous laparotomy wound, about 0.1 million women acquired a horizontal abdominal scar from a cesarean section in 2015. Because the proportion of nulliparous women aged 35 or older is continuously increasing, it is anticipated that the number of women who will suffer from scarring after a cesarean section will continue to grow.
Most steps utilized during a cesarean section are evidence-based, and are comparable throughout the world [34]. Among the available abdominal incisions used for a cesarean section, a Pfannenstiel incision is selected most frequently, and achieves superior cosmetic results compared with a vertical incision [5]. With this type of incision, the skin is usually closed using subcuticular sutures or staples, both of which are known to result in similar final cosmetic outcomes, although a suture is more time-consuming and less prone to wound separation [6789].
Cochrane review by Alderdice et al. [10] concluded that there was no conclusive evidence in the choice of techniques and materials to use at skin closure after cesarean section. Reduced mechanical tension, eversion of edges after adaptation, and absence of skin mark by suture material are necessities for good skin closure [11]. Conventional subcuticular suture is considered to be useful for closing wounds with equal tissue thickness and in which virtually no tension exists [12]. However, it is prone to tension being created across the edges of the skin because it does not hold each stitch. Approximation of the edges is also not fully everted when the suture verges on different level of each subcuticular space. It leaves marks at midline and both ends. The buried intradermal suture or the intradermal buried vertical mattress suture with absorbable material seems to be fulfilling above mentioned criteria for better wound healing [13].
The aim of this study is to compare the subcuticular suture with the intradermal buried vertical mattress suture for the cosmetic outcome of the scar and the level of overall satisfaction of the patient.
Materials and methods
Cases were recruited from all cesarean sections performed in 2015 at the Pusan National University Yangsan Hospital. A conventionally applied subcuticular suture for skin closure after a cesarean section was replaced with the intradermal buried suture on June 16, 2015. Due to the fact that this change was not originally designed for prospective study and lack of enough evidence regarding better cosmesis of different skin closure method, no comment was given to patients about the possible cosmetic advantage that newer method might have over conventional one.
A total of 303 cesarean section using a Pfannenstiel incision was utilized in our study. Patients with a previous cesarean section or having a suprapubic transverse laparotomy history were included regardless of their number of previous surgeries. Elective or emergent cesarean sections were both included.
To eliminate ethnic variations, non-Korean patients were excluded. Patients having uncertain medical records regarding the skin closure method applied were also excluded. Nine of the women were excluded based on their non-Korean ethnicity, i.e., 4 Chinese, 2 Vietnamese, 1 Cambodian, 1 Laotian, and 1 Indonesian. Three patients were also excluded because of poor medical records, which did not indicate the skin closure method applied. By reviewing the charts, we excluded cases of neonatal deaths or severe morbidities. Therefore, a total of 23 patients were removed from the list owing to a fetal issue, and 2 were subtracted for maternal reasons, i.e., one for a severe peripartum hemorrhage requiring uterine arterial embolization, and one because of postpartum depression.
For the control group used in the present study, the skin closure method applies subcuticular stitch using a non-absorbable monofilament suture made of polyamide polymers, size 3 (Ailee, Busan, Korea). Buried knot intermittent intradermal stitch using a synthetic absorbable braided suture made of polyglactin 910, size 4 (Ethicon, Johnson & Johnson International, New Brunswick, NJ, USA) was applied to the test group. For both groups, the wound was reinforced using a Steri-Strip (Johnson & Johnson International), and patients were advised to remove them on postoperative day 7. The scar is then covered with a 10×20 cm Mepilex Border (Mölnlycke Health Care, Gothenburg, Sweden) until postoperative day 1. According to a critical pathway program for cesarean sections, the patients are encouraged to discharge on postoperative day 3. Stitch removal, applied only to the control group, was conducted on postoperative day 7 at an outpatient clinic.
Suturing technique of the intradermal buried vertical mattress is well described in the study of Hohenleutner et al. [13]. First, the needle should be inserted in the lower part of dermal layer or the superficial subcutaneous tissue. Then it drives upwardly toward skin to make perpendicular arch and is brought out at the top of the epidermis. In the opposite edge, it courses the same but is directed inversely; entering into just below the epidermis, passing vertically toward dermis and exiting the dermis at the same depth of the initial insertion site. The suture encompassed only small portion of fatty tissue of subcutaneous layer and the edges were gently everted. Fig. 1 demonstrates intradermal buried vertical mattress suture.
Fig. 1
Intradermal buried vertical mattress suture. (A) Initial suture approaches from low part of epidermis. Please note that suture encases epidermis only, or a including very small proportion of subcutaneous fat. (B) Please note the buried knot and slightly everted edge.

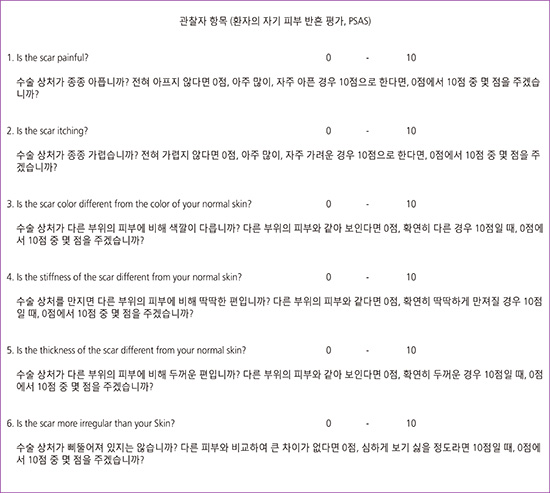
A scar assessment was conducted through a telephone survey, with the calls made on a weekday between 9 a.m. to 5p.m. The patient component of the patient and observer scar assessment scale (POSAS) was utilized along with the overall satisfaction of the patient regarding their cesarean section scar and their willingness to choose the same skin closure technique when anticipating their next cesarean section. The patient scar assessment scale (PSAS) includes 6 variables: 1) pain and 2) pruritus around the scar, and the 3) color, 4) stiffness, 5) thickness, and 6) irregularity as compared to the adjacent normal skin (Fig. 2). Each variable has a score of 1–10, with 10 representing the worst wound conditions. The PSAS was translated into plain Korean (Appendix 1), but the translation was not validated. The patients were asked to participate in this study voluntarily. We proceeded with each interview only after obtaining verbal approval of the patient. The period between the date the cesarean section was conducted and the telephone interview was 12–18 months.

The PSAS and overall satisfaction scores of each group were analyzed using a Student's t-test and a Wilcoxon rank-sum test (Mann-Whitney U test), respectively. A P-value below 0.05 was considered statistically significant. A Pearson's χ2 test and logistic regression were used to evaluate the preference toward a specific skin closure method. The Pearson's correlation coefficient was calculated based on the PSAS score and level of overall satisfaction. The statistic power of this study was relatively low: the 50 patients used in each group and a PSAS score of 6 for the difference in interest provided a power of 59.5% with a level of significance of 5%. This low power is considered to have originated from the large deviation in PSAS scores, the reason for which is discussed later. All data analyses were conducted using R statistical program, ver. 3.3.1 (R Foundation, Vienna, Austria; http://www.R-project.org/), an open-source programming language for statistical computing.
Results
We called 266 patients. Seven were unable to be contacted because we had the wrong number on file. Over 50% of the patients (n=149) did not answer our call. Among the responders, five refused to be interviewed and 2 had an additional repeat cesarean section. A total of 103 patients finished the survey, but one was excluded from the final analysis owing to a history of keloids. The response rate was 38% (102 out of 266). Subcuticular stitch using a non-absorbable monofilament suture was applied to 52 of the patients (control group), and 50 patients underwent intradermal buried vertical mattress using a synthetic absorbable braided suture (test group). A flow chart of the telephone survey conducted is shown in Fig. 3.

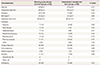
The demographic characteristics of the groups are summarized in Table 1. Both groups showed similar baseline characteristics. The operation time was slightly longer for the test group, but with no statistical significance. We did not exclude diabetic patients from the analysis, and data on the wound complications were not collected for review in this study.
Table 1
Demographic characteristics
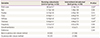
The results of the scar assessments are shown in Table 2. The PSAS score of the test group was lower than that of the control group, with a statistical significance (P=0.02). Mean PSAS score was 28 in control group, whereas 21.8 in test group (P=0.02). In each PSAS variables, scores of pain, pruritus, and irregularity did not show statistically significant difference between the groups. Changes in color, stiffness and thickness of scar tissue comparing to adjacent normal skin of the test group showed significantly better results than those of control group; these in sum might have played pivotal role in showing significant difference in total PSAS scores. In both groups, 2 variables of pain and pruritus tended to be lower than the other 4 variables. The overall rate of satisfaction was slightly higher in test group, but it was not statistically significant (P=0.69).
Table 2
Scar assessment results
Correlation between the PSAS score and the level of overall satisfaction was calculated by the Pearson's correlation coefficient. As patients reported lower PSAS scores, they tended to have higher satisfaction (P<0.1). Fig. 4 represents the PSAS plot based on the overall level of satisfaction at the original scale. Personal preference did not differ between the 2 groups.

Discussion
Our results indicate a significant difference in the final cosmetic outcomes according to the skin closure method. Intradermal buried vertical mattress using synthetic absorbable braided sutures showed better cosmesis than conventional subcuticular stitch using non-absorbable monofilament sutures. The overall level of satisfaction was also slightly higher in the test group than in the control group, but without a statistical significance. It should be highlighted that our results are based on the patient’s own judgment regarding their abdominal scar. A very significant correlation between the PSAS and overall level of satisfaction implied a strong reliability. However, personal preference was not affected by the specific suture methods applied.
In our study, patients reported low scores in pain and pruritus of the scar comparing to other PSAS components in both groups. They are the acute component of wound complications and reflect the time elapsed from the surgery to the reporting. Correspondingly, aggravated scores in color, stiffness, and thickness in the control group implies that chronic wound complications are perceived better by patients themselves in the test group. This result also supports reliability of the patients-derived scar assessment system utilized in this study. At the same time, these chronic components should be highlighted when comparing cosmetic outcomes of surgical scar.
At the Pusan National University Yangsan Hospital, a conventionally applied procedure for skin closure following a cesarean section was replaced with a more delicate method on June 16, 2015. Complaints regarding hypertrophic scar and pain or pruritus at the scar site motivated this change. Although intermittent stitch covering at least a 15 cm long horizontal incision seemed time-consuming, we started its application to achieve better wound healing. As discussed earlier in this paper, we hypothesized that intradermal buried vertical mattress may reduce tension across the wound. During the wound healing process, both local and systemic factors are important [14], and mechanical tension on the wound has been identified as a leading cause of hypertrophic scarring [15].
A standardized scar assessment is a crucial aspect of this study. Although an objective method such as spectrophotometry may be ideal, many studies are still focusing on subjective methods using scar-rating scales [16171819]. The Vancouver scar scale (VSS) has been the most commonly used approach in scientific studies on scarring [20]. The POSAS was introduced by Draaijers et al. [21] in 2004 and achieves a slightly better reliability than the VSS [20]. The patient's own judgment of the POSAS has brought about an important improvement over other subjective scar assessments [22].
At the beginning of this study, we anticipated 2 major drawbacks: the lengthy time-gap between surgery and the evaluation of the scar appearance, and physician-excluded scar-rating scores. Most comparison studies consider the end point of a scar assessment to be between 2 to 6 months post-operation [16171819]. Wound healing begins with hemostasis and ends with tissue remodeling. Wound maturation can last for a year or longer, depending on the wound type [23]. In this study, more than a one-year time-gap exists between scar creation and reporting. This is considered a virtue for the present study because it allows the final configuration of the scar to be shown. Cromi et al. [19] reported that the time interval between surgery and scar assessment did not significantly influence the patient's opinion of their scar. Furthermore, the color, stiffness, thickness, and irregularity of the scar when compared with the adjacent normal skin are not believed to influence their memory because the patient can see and feel their wound daily. Brown et al. [24] reported that the correlation between psychosocial distress and objective scar severity was not significant. The effect of a scar on the daily life of a patient in terms of personal distress is not necessarily proportional to its size. This study highlights the patients' personal scar assessment. Scarring has the potential to devastate one’s self-esteem and can be a source of distress in younger people [25]. When measuring the cosmetic outcomes of a cesarean section scar, one should try to evaluate the patient's own opinion. We attempted to determine how much the patients have contended with regarding their cesarean scars.
The reporting pattern should also be considered. Both extremes of the PSAS scores made up too large a proportion of the total scores. Fifteen patients reported 6–9 points for total PSAS score where the minimum was 6. Eighteen scored the same or above 40 out of maximum score of 60. By removing these two extremes, the standard deviation of the PSAS scores decreases from 13.5 to 8.5, which in turn increases the power of this study from 59.5% to 93.7%. This all-or-none pattern could be explained that patients tend to judge their wound in holistic fashion. Although patients are supposed to answer to each variable in the questionnaire accordingly, but it seemed that each variable had influenced others. Interestingly, Gaertner et al. [17] reported a much wider spread in scores when women evaluated their own scar as compared to the evaluation by examiner. Cromi et al. [19] also reported that the POSAS had narrow deviation compared to the PSAS and they were adjustable with observer scales of the scar assessments, such as VSS and POSAS.
Schema of staples versus subcuticular sutures were most commonly applied in the previously reported studies regarding skin closure after a cesarean section. Variations are including, but not limited to, suture materials and closure or non-closure of subcutaneous space. Unlikely to others, we focused on stitch techniques rather than different materials used in skin closure, such as staple and suture material. Few study utilized buried knot for skin closure after a cesarean section. We sought to evaluate different types of suture that might impact the final cosmesis. Employing standardized skin assessment scales for numerification of skin appearance and assessing the wound at least 6 months apart from skin closure are similarities between our study and others.
Our study has some potential limitations. First, blindness was not achieved during the phone call survey. Some of the interviewers were able to know the type of skin closure method applied based on the date of the cesarean section recorded on the patient list. Second, patients who are content or discontent with another aspect of their surgery may have been accordingly biased in reporting their scar assessment. Third, we dismissed the relation between wound healing and a systemic condition such as diabetes [26]. Fourth, although we applied different skin closure materials to the 2 study groups, the possibility of their implication on the cosmesis was not evaluated. Absorbable and non-absorbable suture material did not have significant impacts on wound healing and wound complication [27].
In conclusion, we suggested the use of intradermal buried vertical mattress using synthetic absorbable braided sutures as a cosmetically superior skin closure method for application in cesarean sections over conventional subcuticular stitch with non-absorbable monofilament sutures. The use of the proposed stitch does not significantly increase the operation time. To validate this result, a randomized trial with sufficient statistical power should be conducted. Ultimately, such comparison should encompass staples and different suture materials, allowing an evidence-based skin closure method with a better cosmetic outcome to be made available in the near future.
 XML Download
XML Download