

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Considering the effects on perinatal morbidity and mortality, preterm labor is one of the most important problems in obstetrics, accounting for more than one-third of all preterm births [12]. So far, ritodrine and magnesium sulfate are the most commonly used tocolytics for preterm labor. Ritodrine is an approved drug by Korean Food and Drug Administration and is the most commonly used medication as a tocolytics. However, side effects such as palpitations, pulmonary edema, hands tremors, hypokalemia, and hyperglycemia are known to occur [34]. The Magnesium sulfate is not approved for tocolytics and is used as an off-label drug for a preterm labor, in addition to other purposes such as prevention of eclampsia and prevention of cerebral palsy in premature infants [5]. Magnesium sulfate may also cause side effects such as nausea and vomiting, lethargy, dyspnea, headache, hypotension, and dizziness [156]. Therefore, it may be needed to evaluate the safety of magnesium sulfate in comparison with ritodrine.
In terms of efficacy to inhibit uterine contractions, several previous studies have shown that the success rate in inhibiting preterm labor (within 48 hours or within 7 days) was not different between magnesium sulfate and ritodrine [278]. However, there is a paucity of information regarding the efficacy of both medications after consideration of intra-amniotic infection, although numerous data suggest that intra-amniotic infection is one of the most important prognostic factors in patients of threatened preterm birth [91011].
The objective of this study was to compare the efficacy and safety of magnesium sulfate with that of ritodrine in preterm labor, and to analyze the factors affecting the efficacy of the drug in patients for the treatment of preterm labor.
Materials and methods
1. Study population
In this retrospective study, pregnant women who were treated with tocolytics (ritodrine or magnesium sulfate) with the diagnosis of preterm labor (24–33.6 weeks of gestation) and underwent amniocentesis to evaluate the presence of infection in the amniotic fluid or fetal lung maturation in Seoul National University Hospital were included between January 2005 and April 2015. Women diagnosed with premature rupture of membrane or pre-eclampsia were excluded. The study population was divided into ritodrine group and magnesium sulfate group according to the type of first-line tocolytics.
2. Definition
Preterm labor was defined as regular uterine contractions, and the choice of first tocolytics drug and the administration dosage of tocolytics was at the discretion of attending physician. Usually ritodrine was administered with an initial dose of 6.4 mg/hr with increment of 3.2 mg/hr every 15 minutes until the cessation of uterine contractions, and magnesium sulfate was given as a 0.004–0.006 g loading dose followed 1.2–3 g/hr of maintenance dose.
The efficacy of tocolytics was assessed in terms of inhibition of preterm birth within 48 hours, within 7 days, or within 37 weeks of gestation, and the frequency of changing to the second-line therapy was also evaluated. To compare the efficacy of both medications with consideration of other clinical factors, the patients were divided into treatment success group and failure group according to whether they were delivered within 48 hours or not. The gestational age of initiation of tocolytics administration, the gestational age of delivery, the frequency of second-line therapy needed, the duration of medication, the rate of twin pregnancy, maternal age, parity, the presence or absence of amniotic fluid infection, and maternal C-reactive protein (CRP) were compared between 2 groups of cases.
The side effects of the drugs were analyzed in women who used only one tocolytics, and women who needed second-line therapy were excluded from the analysis of side effects. In terms of adverse events, the tachycardia was defined as heart rate exceeding 110 rate/min, the tachypnea was defined as respiration rate exceeding 20 times/min, and the hypokalemia was defined as a plasma potassium level of less than 3.0 mEq/L. Hyperglycemia was defined as the state of above 200 mg/dL blood sugar level regardless of diet. Amniotic fluid infection was defined as a positive result in amniotic fluid culture.
3. Statistical analysis
Statistical analysis was performed using SPSS 23.0 for windows (IBM Corp., Armonk, NY, USA). Mann-Whitney U test was used to examine the differences between the 2 groups in terms of the continuous variables. The χ2 test was used to compare proportions. Multivariate logistic regression was done for analysis risk factors for treatment failure on the basis of significant factor affecting efficacy of tocolytics. P-value <0.05 was considered statistically significant.
Results
1. Clinical characteristics
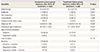
A total of 201 pregnant women were analyzed. Among them, 177 patients (88.1%) were treated with ritodrine and 24 patients (11.9%) were treated with magnesium sulfate. Magnesium sulfate was considered as a first-line therapy especially for patients whose underlying status was hyperthyroidism, cardiac disease or diabetes. Table 1 shows the patient characteristics of study population. There was no significant difference in the maternal age, gestational week at treatment, maternal CRP, and proportion of twin pregnancy, steroid use, positive amniotic fluid culture between the 2 groups of cases. However, there was a difference in parity between the 2 groups (P=0.020).
Table 1
Patient characteristics

![]()
2. Efficacy evaluation between ritodrine and magnesium sulfate
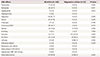
Table 2 shows the efficacy of both tocolytics. Gestational age at delivery, median duration of therapy, preterm delivery within 48 hours, 7 days, or 37 weeks, and the need for 2nd line therapy were not significantly different between the two groups of cases though the rate of delivery after 37 weeks (ritodrine group=14.8% and magnesium sulfate group=4.2%) was lower and need for 2nd line therapy (ritodrine group=7.3% and magnesium sulfate group=12.5%) was higher in magnesium sulfate group.
Table 2
Efficacy of ritodrine and magnesium sulfate

![]()
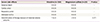
To evaluate clinical factors which determine preterm delivery within 48 hours of treatment, study population was divided into 2 groups according to the occurrence of preterm delivery within 48 hours of treatment; treatment success group (patients who delivered after 48 hours of treatment) and treatment failure group (patients who delivered preterm within 48 hours of treatment). The type of tocolytics was not significantly associated with treatment failure. In addition, there was no significant difference in the maternal age, parity, and steroid use between treatment success group and treatment failure group (Table 3). However, patients in treatment failure group had higher gestational age at treatment and maternal CRP, and higher proportion of twin pregnancy and positive amniotic fluid culture than those in treatment success group.
Table 3
Characteristic difference according to the efficacy of tocolytics
![]()
In multivariate analysis, type of first-line tocolytics was not associated with treatment failure even after adjustment for confounding factors. In the multivariate logistic regression model, gestational age of tocolytics administered, twin pregnancy, positive amniotic fluid culture, and maternal CRP were significant risk factors for treatment failure (Table 4).
Table 4
The relationship between various clinical factors and tocolytics treatment failure, analyzed by multiple logistic regression analysis

![]()
In study population, 14 patients (7%) showed positive amniotic fluid culture result. The culture microorganisms were Ureaplasma (8 cases), Mycoplasma, Escherichia coli, Candida, Gardnerella, and Streptococcus (polymicrobial invasion was present in 3 cases). Table 5 compares the clinical characteristics and pregnancy outcomes according to the result of amniotic fluid culture. Patients with positive amniotic fluid culture had higher maternal CRP levels and had higher risk of preterm delivery (within 48 hours and with 7 days) than those with negative amniotic fluid culture.
Table 5
Clinical characteristics and pregnancy outcomes according to the result of amniotic fluid culture

![]()
3. Maternal side effects
Patients who needed both ritodrine and magnesium sulfate for tocolysis as first line and second line therapy were excluded from the analysis of side effects. The side effect of the first-line therapy was compared between the ritodrine group of 164 patients and magnesium sulfate group of 21 patients. In the group using ritodrine, several side effects were occurred in the order of palpitations (81.7%), hand tremor (57.9%), tachycardia (47.0%), chest discomfort (34.1%), tachypnea (20.7%), and nausea (14.6%). In the magnesium sulfate group, the common side effects were burning sensation (76.2%), lethargy (66.7%), dizziness (47.6%), and nausea (19.0%). When ritodrine was used, side effects such as palpitations, hand tremor, tachycardia, chest discomfort, and tachypnea were significantly more frequent, and when magnesium sulfate was used, facial flushing, lethargy and dizziness were more significantly increased than in ritodrine group (Table 6). The probability of occurrence of one or more side effects was 93.9% for ritodrine group and 90.5% for magnesium sulfate group (P=0.630).
Table 6
Type of side effect of ritodrine and magnesium sulfate
![]()
In terms of severe side effects, the first-line tocolytic treatment was discontinued in seven patients (4.2%) in ritodrine group and two patients (9.5%) in magnesium sulfate group because of intolerable side effects of the drug (P=0.271, Table 7). The causes of discontinuation of the treatment in the ritodrine group were chest discomfort (3 cases), palpitation (3 cases) and pulmonary edema (1 case). In the magnesium sulfate group, the causes of discontinuation of the treatment were lethargy which may make it difficult to open the eyes (1 case) and chest discomfort (1 case). The longer duration of tocolytics treatment (for more than 48 hours) was not associated with the discontinuation of therapy because of maternal adverse outcome (3.3% in patients who were treated with tocolytics for more than 48 hours vs. 7.1% in patients who were not).
Table 7
Severe side effect of ritodrine and magnesium sulfate
![]()
No severe maternal complications such as maternal death, cardiac arrest, respiratory arrest, and intensive care unit admission were occurred in both groups.
Discussion
The principal finding of the current study was; 1) The efficacy (preterm delivery within 48 hours, 7 days, or 37 weeks of gestation and need for 2nd line therapy) was not different between ritodrine and magnesium sulfate; 2) In multivariate analysis, gestational age at treatment, twin gestation, intra-amniotic infection and maternal CRP was associated with treatment failure (preterm delivery within 48 hours), but the type of tocolytics was not significantly associated with treatment failure; 3) The type of side effect was different in the 2 groups, but the frequency of total adverse effect, need for discontinuation of therapy because of maternal adverse effect, and severe adverse effect were not different between the 2 groups of cases.
Until now, several medications have been used in preterm labor, and ritodrine and magnesium sulfate are the most frequently used tocolytics [4712]. Magnesium sulfate is known to suppress the uterine contraction by antagonism to calcium ions [5]. Ritodrine is a β-adrenergic agonist that binds to β-sympathetic receptors in the uterine smooth muscle cell membrane and relaxes the uterine smooth muscle by decreasing the concentration of calcium that causes muscle contraction [12]. However, the problem with β-adrenergic agonists is that β-sympathetic receptors are distributed not only in the uterine muscle but also in the vascular wall, resulting in unintended side effects. The side effects caused by this include maternal cardiovascular side effects, hypokalemia, and hyperglycemia. The most common side effects of ritodrine administration are tachycardia, hypotension, and chest discomfort, but uncommon fatal side effects such as pulmonary edema and myocardial infarction have been reported [13].
In this study, the safety and efficacy of magnesium sulfate, as an alternative tocolytis, was compared with that of ritodrine. As a result of specific mechanism of action of both tocolytics, side effects related with vital signs such as palpitations, hand tremor, tachycardia, chest discomfort, and tachypnea were significantly more frequent in ritodrine group whereas facial flushing, lethargy, and dizziness were much significantly occurred in magnesium sulfate group. The overall side effects showed different frequency of incidence according to each drug use, but there was no difference in severe side effects, in terms of discontinuation of drug use due to severe side effects and the fatal maternal side effects (maternal death, cardiac arrest, respiratory arrest, and intensive care unit admission). Therefore, it can be concluded that ritodrine and magnesium sulfate are similar in terms of safety.
In addition, in order to evaluate the efficacy of the tocolytics, treatment success (delay of delivery within 48 hours after drug administration) was analyzed. The type of first-line tocolytics (ridodrine vs. magnesium sulfate) was not significant determinant of treatment failure. Therefore, we might conclude that magnesium sulfate as a tocolytics in preterm labor patients is not different from ritodrine in terms of efficacy.
There have been several studies which showed that that the efficacy was not different between magnesium sulfate and ritodrine [34]. Recently, Hwang et al. [13] reported multicenter study on the practice pattern in management of threatened preterm labor in Korea. In this study, the effectiveness of ritodrine and magnesium sulfate was similar and the poor tolerance to therapy was comparable between the 2 tocolytics, and these results are consistent with the result of the current study. However, the comparison of efficacy after adjustment for intra-amniotic infection has not been well determined, although numerous studies have suggested that intra-amniotic infection is the major risk factor of preterm delivery [91011]. In the current study, the efficacy of treatment success was not related to the type of first-line tocolytics, but was influenced by the gestational age of tocolytics administered, twin pregnancy, amniotic fluid infection, and maternal CRP.
This study was based on the retrospective study with patients who underwent amniocentesis among the inpatients due to preterm labor. Therefore, the number of magnesium sulfate used group was relatively small, and the decision on type of tocolytics was at the discretion of attending physician which might result in different indications for both tocolytics and in selection bias (for example, magnesium sulfate might be used as a first-line therapy especially for patients with medical disease such as hyperthyroidism, cardiac disease, or diabetes). Further studies through prospective randomization studies may be needed to evaluate the efficacy and safety of magnesium sulfate.
And about magnesium sulfate, there are 2 more important points. Magnesium sulfate has a neuroprotective effect for preterm birth before 32 weeks of gestation. So we should consider magnesium sulfate especially for patients who have high risk for preterm birth within 32 weeks [5]. In addition, the concerns on its adverse effect of fetal bone should be kept in mind in patients who need magnesium sulfate for more than 7 days [14].
In conclusion, the efficacy and safety of magnesium sulfate was similar to ritodrine, and can be a substitute tocolytics. Additionally, failure of tocolytic therapy was determined by gestational age at treatment, twin gestation, intra-amniotic infection and maternal CRP, not by the type of tocolytics.
 XML Download
XML Download