

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Urinary incontinence (UI) is defined as involuntary loss of urine, which is a social or hygienic problem according to the International Continence Society [1]. UI is considered as a chronic disease with a high incidence [2]. Stress urinary incontinence (SUI) is UI that occurs suddenly owing to increased abdominal pressure from exercises, sneezing, or coughing. This is because the pressure on the bladder, which is increased by abdominal pressure, is higher than the pressure of the urethral sphincter, which prevents urine leakage. SUI can be managed conservatively, mechanically, pharmacologically, or surgically. Among the surgical treatments of SUI, the midurethral sling, which was introduced in 1996, is the most common type of surgery used to correct SUI in a minimally invasive manner. After the tension-free vaginal tape (TVT) was introduced, it became widely used in surgery for SUI [3]. TVT is used in simple procedures, and it is associated with few complications, such as occlusive nerve injury, retropubic hematoma or abscess, chronic urinary retention, vaginal wall and urethral erosion, and colorectal injury. To reduce the risk of these complications, the transobturator tape (TOT) procedure, in which the tape is passed through the obturator foramen, was introduced [4].
The prevalence of UI increases with age and for woman who have had previous births. In addition, the prevalence of UI is higher in women who have had previous vaginal delivery than in those who have undergone cesarean section [5]. Studies have shown that smoking and caffeine may increase the risk for incontinence [6]. Obesity is also a well-known risk factor for UI that affects the progression and recurrence of disease [7]. Obese status may lead to increased abdominal pressure [8] and cause UI by compressing the bladder. Additionally, obesity may cause increased intra-abdominal pressure and expose the pelvic support structures and organs to a chronic state of stress, and pelvic floor muscle fatigue may develop secondary to this increased pressure [9]. The purposes of this study were to examine the clinical outcome of obesity in women who underwent the TOT procedure for SUI, and to compare the differences in postoperative urinary symptoms between average-weight women and obese and overweight women.
Materials and methods
This retrospective cohort study was conducted in patients who underwent the TOT procedure for SUI at the Department of Obstetrics and Gynecology of Yonsei University Severance Hospital from January 2006 to October 2011. Patients who received follow-up care less than 1 year or previously underwent incontinence surgery were excluded from this study.
The primary outcome was the occurrence of urinary symptoms. Patients' characteristics were obtained by review of their medical records.
Patients were requested to report the presence of urinary symptoms, including leakage, frequency, urgency, voiding difficulty, hesitancy, post-void residual urine, constipation, and dyspareunia, preoperatively in the outpatient clinic. Obstetric history such as the times of delivery, menopausal status, and history of hormone therapy were also reported by the patients. Moreover, a physical examination was conducted to confirm anatomical and nerve abnormalities. All patients underwent pelvic examination by a physician in the lithotomy position to evaluate pelvic organ prolapse, including uterine prolapse, enterocystocele, and proctocele. We performed a stress test, measured urethral hypermobility using the Q-tip test, and conducted a urodynamic study in all patients. Patients who were diagnosed as having stress incontinence through the urodynamic study underwent the TOT procedure. The TOT used in the surgery was the Gynecare TVT Obturator System (Johnson and Johnson, New Brunswick, NJ, USA).
Body mass index (BMI) was calculated as the patient's weight in kilograms divided by the patient's height in meters, squared. Patients were divided into four groups according to BMI: normal weight (BMI, 18.5 kg/m2), overweight (BMI, 23.0 kg/m2), obese 1 (BMI, 25.0 kg/m2), and obese 2 (BMI, 30.0 kg/m2 or higher). We compared the risk of postoperative outcomes after the TOT surgery among the four groups. For BMI 30.0 or over, the number of patients were small but it was acknowledged to be more meanigful to analyze by caterotizing the patients as severe obese.
Postoperative follow-up interviews were performed to evaluate patients' postoperative status. After the TOT procedure, patients answered the question items and confirmed their status of urinary leakiness, frequency, urgency, voiding difficulty, hesitancy, post-void residual urine, constipation, and dyspareunia. Patients complaining of urinary symptoms postoperatively were followed up after prescription of medication depending on their symptoms. Data was analyzed by χ2 test, Fisher's exact test and reported as a value of number (%).
This study was approved by a certified Institutional Review Board, at Human Research Protection Center, Yonsei University Severance Hospital (assignment number: 4-2017-0573).
Results
From January 2006 to October 2011, we reviewed 310 patients who were diagnosed as having SUI and underwent the TOT procedure at the Department of Obstetrics and Gynecology of Yonsei University Severance Hospital. Among these patients, 281 received the follow-up care for more than 1 year. Eighty-nine (34%) patients were classified as normal weight (BMI, 18.5–22.9 kg/m2), 78 (25%) as overweight (BMI, 23.0–24.9 kg/m2), 101 (37%) as obese 1 (BMI, 25.0–29.9 kg/m2), and 13 (3%) as obese 2 (BMI, 30.0 kg/m2 or higher). There was no significant difference in patients' age, the menopausal status at the time of surgery, and whether they had received previous hormone therapy between the groups. There was also no significant difference in the type of delivery, namely vaginal parity, status of home delivery, and status of difficult labor between the four groups (Table 1). Patients in all groups reported that their symptoms improved postoperatively. None of the patients required reoperation because of postoperative urinary symptoms.
Table 1
Characteristics of study population
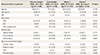
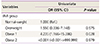
Regarding postoperative urinary symptoms, the obese group had a higher occurrence rate than the other groups. Postoperative urinary symptoms, including urine leakage, frequency, urgency, voiding difficulty, hesitancy, weak stream, post-voiding residual urine, and dyspareunia, occurred in 3.4% (n=3) of normal-weight women, 5.1% (n=4) of overweight women, and 12.9% (n=13) of obese 1 women (P=0.038) (Table 2). The risk of postoperative urinary symptoms after TOT surgery was almost four times more likely to occur in the obese 1 group than in the normal-weight group (odds ratio, 4.235; P=0.028) (Table 3).
Table 2
Postoperative urinary symptoms

Discussion
SUI has a significant effect on the quality of life and mental aspects of women. We found that postoperative urinary symptoms after TOT procedure are more likely to occur in overweight women than in normal-weight women. The increase of BMI is closely related to the increase in abdominal pressure, and obesity has a significant effect on the recurrence of SUI [10]. Subak et al. [11] conducted a 6-month weight loss program for overweight and obese women with urinary leakage symptoms. The authors concluded that 226 women with an average weight loss of 8.0% experienced a 47% reduction in the episodes of incontinence. It was suggested that weight loss in overweight and obese women can be helpful in reducing the symptoms of UI [11]. Auwad et al. [12] revealed that if obese women lose 5% of their body weight, they can experience significant improvement in UI and quality of life. However, further research is needed to confirm whether decreasing one's weight after the TOT procedure will help lower the recurrence of postoperative urinary symptoms. Additionally, in our study, there were more urinary symptoms after the TOT procedure in obese patients. Further, these patients should be studied to compare the improvement of urinary symptoms before and after weight management.
According to Cummings et al.'s statement [13], the sling operation is a good surgical treatment for morbidly obese women. Likewise, in our study, the patients showed improvement of symptoms of SUI, and no patients required reoperation after TOT surgery. However, a study conducted by Hellberg et al. [14] showed that morbidly obese women who underwent the TVT procedure for SUI were more likely to experience unfavorable results. As obesity increases, the cure rate is more likely to decrease. In a study of 970 patients who underwent the TVT procedure, 291 with normal weight had a cure rate of 81.2%; in contrast, only 61 morbidly obese woman (BMI >35.0 kg/m2) had a cure rate of 52.1% [14]. The authors found that obese women had more urinary symptoms postoperatively when compared with the normal-weight women. In our study, postoperative urinary symptoms were significantly more frequent in obese patients than in the other patients, but there was no difference in each of the three symptoms, i.e., urine leakage, frequency, and urgency.
The strength of this study is that we observed the postoperative urinary symptoms of the patients who underwent the TOT procedure for SUI within 1 year postoperatively. Until now, no researchers have followed up on the symptoms of patients for months and compared the symptom occurrence before and after surgery. We compared the occurrence of postoperative urinary symptoms between levels of obesity. The limitation of this study is that the number of patients with BMI >30.0 kg/m2 was substantially lower than the number of patients in the other BMI groups; therefore, it is difficult to make comparisons among morbidly obese women.
In conclusion, TOT seems to be a good treatment choice for SUI regardless of the patient's BMI. This study's findings indicate that if patient undergoing the TOT procedure is obese, urinary symptoms are more likely to occur frequently after surgery. Weight reduction before the TOT procedure can improve patients' postoperative urinary symptoms.
 XML Download
XML Download