

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
It has been proposed that antiphospholipid antibodies (APAs) may have some relationship with infertility and in vitro fertilization (IVF) outcomes [1].
From the literatures, the prevalence of positive APA ranged from 0% to 11.4% in healthy or fertile women, from 3.3% to 23.7% in unexplained infertility, and from 0% to 66% in women undergoing IVF [2345678910111213]. From 54 Korean women undergoing IVF due to tubal factor, the prevalence of APA was 16.7% [14].
In women with IVF failure, the prevalence of positive APA ranged from 4.2% to 30.4%, but it was 0% in women conceived or delivered after IVF [11012]. In women with 3 or more failed IVF, the prevalence ranged from 6.0% to 65.9%, in contrast, it ranged from 0% to 33% in women conceived within 2–3 IVF cycles [378]. Collectively, the prevalence of APA was higher in infertile women than fertile control and the presence of APA appears to be associated with IVF failure.
In 2008, American Society for Reproductive Medicine (ASRM) announced that there is no association between APA and pregnancy rate or live birth rate after IVF [15]. They identified 16 literatures in which the pregnancy rate or live birth rate after IVF treatment in APA-negative and APA-positive women were examined. The pooled clinical pregnancy rate and live birth rate were 57% and 46% in APA-positive group and 49.2% and 42.9% in APA-negative group, respectively. They concluded that assessment of APA is not recommended among couples undergoing IVF, and the therapy is not justified. A subsequent meta-analysis including 7 studies also showed that there is no significant association between APA and clinical pregnancy or live birth in patients underwent IVF [16].
However, in a recent retrospective study, APA positivity was associated with significantly lower pregnancy rate and higher abortion rate after IVF [17]. As far as we know, there has been only one report with regards impact of APA positivity on IVF outcomes in Korean infertile women; pregnancy rate was similar between APA-positive and APA-negative group in infertile women who underwent IVF in Korea, however, abortion rate was significantly higher in APA-positive group (62.5% vs. 20.0%) [14].
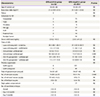
It would be very important whether APA-positive women have poorer IVF outcome. If this is true, immunotherapy should be considered in APA-positive women prior to IVF. As shown in Table 1, the majority of previous studies included women who underwent IVF irrespective of number of previous cycles or women with 2 or more failed IVF cycles. When an association of APA positivity with pregnancy results after IVF is directly assessed, women who underwent the first IVF cycle should be included.
Table 1
Literatures about in vitro fertilization (IVF) pregnancy outcomes in women with positive or negative for antiphospholipid antibodies

| Author, year [reference number] | Study group | No. | Positivity | APA-positive vs. APA-negative | ||
|---|---|---|---|---|---|---|
| Pregnancy rate | Live birth rate | Miscarriage rate | ||||
| El-Roeiy et al., 1987 [25] | Women undergoing IVF | 26 | aCL 34.6% | 10.0% vs. 37.5% | 0% vs. 18.8% | NA |
| aPS 26.9% | ||||||
| Gleicher et al., 1994 [26] | Women undergoing IVF | 105 | 27.6% | 32.8% vs. 23.9% | 26.3% vs. 15.8% | NA |
| Sher et al., 1994 [12] | Women undergoing IVF without habitual abortion | 25 | NA | 16% vs. 27% | NA | NA |
| Nip et al., 1995 [10] | Women with unexplained infertility | 30 | 3.3% | 33% vs. NA | 30% vs. NA | NA |
| Women with tubal factor infertility | 50 | 22% vs. NA | 20% vs. NA | |||
| Birdsall et al., 1996 [3] | Women undergoing IVF | 240 | 15.0% | 38.9% vs. 36.1% | 27.9% vs. 25.5% | NA |
| Kutteh, 1997 [8] | Women undergoing IVF | 191 | 18.8% | 35.3% vs. 39.7% | NA | NA |
| Kowalik et al., 1997 [27] | Women undergoing IVF | 525 | 14.9% | 57.7% vs. 49.7% | 46.2% vs. 43.8% | 20.0% vs. 23.7% |
| Eldar-Geva et al., 1999 [23] | Women with 2 or more failed IVF | 56 | 37.0% | 18.8–52.2% vs. 17.3–50% | 6.3–25.4% vs. 9.9–27.7% | NA |
| Chilcott et al., 2000 [6] | Women undergoing IVF | 380 | aCL or LA 23.4% | 15.7% vs. 19.6% | 9.0% vs. 12.0% | 75.0% vs. 62.8% |
| ab2GPI 3.3% | ||||||
| Hornstein et al., 2000 [16] | Women undergoing IVF | 2,053 | 34% | 57% vs. 46% | 49.2% vs. 42.9% | NA |
| Buckingham et al., 2005 [4] | Women undergoing IVF | 99 | aCL IgG 2%, IgM 2% | 31.6% vs. 36.3% | 15.8% vs. 23.8% | NA |
| ab2GPI IgG 10%, IgM 4% | ||||||
| aPS IgG 4%, IgM 0% | ||||||
| Matsubayashi et al., 2006 [28] | Women with 2 or more failed IVF | 44 | 65.9% | 29.4% vs. 33.3% | NA | NA |
| Sanmarco et al., 2007 [29] | Women with 2 or more failed IVF | 101 | 39.6% | 42.7% vs. 41.9% | 32.5% vs. 32.2% | 5.0% vs. 6.5% |
| Lee et al., 2007 [14] | Women undergoing IVF with tubal factor | 54 | LA 1.8% | 20.5% vs. 17.6% | 7.7% vs. 14.1%a) | 62.5% vs. 20.0%a) |
| aCL 14.8% | ||||||
| Zhong et al., 2011 [17] | Women undergoing IVF with tubal factor | 76 | NA | 31.3% vs. 48.6%a) | NA | 32% vs. 15.1%a) |
| Paulmyer-Lacroix et al., 2014 [30] | Women with 2 or more failed IVF | 40 | 20% | 50% vs. 53% | 0% vs. 35.3% | 25.0% vs. 52.9% |
APA, antiphospholipid antibody, NA, not available; LA, Lupus anticoagulant; aCL, anticardiolipin antibody; ab2GPI, anti-b2 glycoprotein I antibody; aPS, anti-phosphatydilserine antibody.
a)P<0.05.
![]()
Here we assessed the prevalence of APA among Korean women who attempted the first IVF cycle and the influence of APA on clinical pregnancy, miscarriage, and ongoing pregnancy in a subsequent IVF cycle.
Materials and methods
This was a prospective observational study including 219 Korean infertile women undergoing their first IVF at the Seoul Maria Fertility Hospital, and the Seoul National University Bundang Hospital (March 2013 to November 2016). Committee approval was validated and informed consent was obtained from all patients before the study (IRB No. B-1302/190-003).
We included women aged 24–44 years who had female factor or unexplained infertility and destined to the first IVF cycle. The indications of IVF were unexplained (n=83), tubal (n=50), ovulatory (n=23), old age (n=18), decreased ovarian reserve (n=15) endometriosis (n=10), or multiple factors (n=20). During the study period, male factor infertility or uterine factor (uterine malformation, intrauterine adhesion) was completely excluded. Women with past or current thyroid disease, endocrine disorders (diabetes mellitus, hyperprolactinemia), immunologic disorders (rheumatoid arthritis, systemic lupus erythematosus), or current obesity (body mass index ≥30 kg/m2) were excluded.
Before starting ovarian stimulation for IVF, plasma concentration of lupus anticoagulant was measured by clot-based method, and anticardiolipin antibody (IgG/IgM) and anti-β2-glycoprotein 1 antibody (IgG/IgM) were measured by enzyme-linked immunosorbent assay method. Measurement of lupus anticoagulant consisted of screening and confirmative test; if the titer from initial screening was more than 51, a confirmative test was performed and lupus anticoagulant was considered as positive if the titer from confirmative test was 1.2 or more. Anticardiolipin antibody and anti-β2-glycoprotein 1 antibody were considered as positive if the titer was 20 phospholipid unit (PLU) or more.
Except 6 women with stimulation cancellation, 213 women underwent ovarian stimulation for IVF by using recombinant or urinary follicle-stimulating hormone with or without luteinizing hormone. Two types of pituitary suppression protocol were used: luteal long protocol of gonadotropin releasing hormone (GnRH) agonist (113 cycles) or flexible GnRH antagonist protocol (100 cycles). After 2 or more follicles had reached a diameter >18 mm, 250 μg of recombinant human chorionic gonadotropin (hCG; Ovidrel®; Merck-Serono, Darmstadt, Germany) was injected. The oocyte was retrieved 35 hours after the hCG injection. Fertilization was considered if 2 distinct pronuclei and a second polar body were visible. The quality of embryos was evaluated by morphological criteria based on the fragmentation degree and the regularity of blastomeres on day 3 after fertilization and classified as 4 grades (with grade A being the top embryo). We assessed blastocyst quality method presented by Gardner et al. [18]. Embryo transfer was performed day 2 to 5 after the oocyte collection. Luteal phase was supported either by daily progesterone injection or vaginal gel (Crinone®; Merck-Serono). Clinical pregnancy was confirmed by the presence of gestational sac(s) with visible fetal heartbeat(s). Ongoing pregnancy was defined if the pregnancy continued after 12 weeks of gestation, and clinical miscarriage was defined if the pregnancy terminated before 12 weeks of gestation.
The prevalence of APA was assessed in 219 women. The association between the presence of APA and pregnancy results was assessed in 193 women who attempted embryo transfer. Twenty-six women did not reach embryo transfer because of stimulation cancellation (n=6), cancellation of ovum pick up (n=1), no oocyte retrieved (n=1), failed fertilization (n=4), or freezing-all-embryo due to high-risk of ovarian hyperstimulation syndrome (OHSS) (n=14). All statistical analyses were performed using IBM SPSS ver. 19 (IBM Co., Armonk, NY, USA). The data were analyzed using the Mann-Whitney U test or Fisher's exact test as indicated. The results were considered significantly different when the P-value was <0.05.
Results
Among 219 women, APA was positive in 13 women (5.9%). Lupus anticoagulant (confirmative test) was positive in 2 women (0.9%). No woman had a positive anticardiolipin IgG antibody, but 7 women was positive for anticardiolipin IgM antibody (3.2%); low titer (20–29 PLU) in 4 women, moderate titer (30–79 PLU) in 2 women, and high titer (>80 PLU) in 1 woman. Anti-β2-glycoprotein 1 antibody was positive in 4 women (1.8%); IgG antibody was positive in 2 women and IgM antibody was positive in 2 women. No women are positive for 2 kinds of APA.
In 193 women entering embryo transfer, clinical pregnancy was noted in 91 women (clinical pregnancy rate per transfer: 47.2%) and twin rate was 27.5% (25/91). Chemical pregnancy occurred in 15 women and ectopic pregnancy occurred in one woman but these were excluded from the assessment of clinical pregnancy rate. Among 91 women with clinical pregnancy, clinical miscarriage occurred in 17 women (clinical miscarriage rate per clinical pregnancy: 18.7%). Sixteen miscarriages occurred among singleton pregnancy and 1 in twin pregnancy. Vanishing twin was observed in 3 women but these were not included into the miscarriage rate.
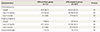
In 193 women entering embryo transfer, clinical characteristics and stimulation outcomes were comparable between APA-positive (n=12) and APA-negative group (n=181) (Table 2). The clinical pregnancy rate (66.7% vs. 45.9%) and ongoing pregnancy rate (58.3% vs. 37.0%) was similar between APA-positive and APA-negative group. Miscarriage rate was also similar between 2 groups (12.5% vs. 19.3%) (Table 3).
Table 2
Clinical characteristics and ovarian stimulation outcomes in women with antiphospholipid antibody (APA)-positive and -negative group
Data shown are median (95% confidence interval). Mann-Whitney U test, χ2 or Fisher's exact test.
NS, not significant; IVF, in vitro fertilization; DOR, diminished ovarian reserve; AMH, anti-Müllerian hormone; GnRH, gonadotropin releasing hormone.
![]()
Table 3
Pregnancy outcomes in women with antiphospholipid antibody (APA)-positive and -negative group
![]()
In 2 women with positive lupus anticoagulant, one woman was pregnant and no miscarriage occurred (clinical pregnancy rate: 50%, ongoing pregnancy rate: 50%).
In 7 women with positive anticardiolipin IgM antibody, embryo transfer was cancelled in one woman because of high-risk of OHSS; among 6 women, 3 women were pregnant and one miscarriage occurred (clinical pregnancy rate: 50%, ongoing pregnancy rate: 33.3%).
All 4 women with positive for anti-β2-glycoprotein 1 antibody were pregnant and no miscarriage occurred (clinical pregnancy rate: 100%, ongoing pregnancy rate: 100%).
Discussion
In the present study, the prevalence of APA was 5.9% among Korean women destined to the first IVF cycle. This prevalence is quite low when considering the result from previous studies (Table 1). The prevalence of each APA was also low when comparing with the result from other reports.
The prevalence of positive lupus anticoagulant in infertile women has been reported to be highly variable ranged from 0% to 17.8% [1]. In our study, lupus anticoagulant was rarely positive (0.9%) among women destined to the first IVF cycle, as like in another report from Korea (1.8% among women undergoing IVF due to tubal factor) [14].
The prevalence of positive anticardiolipin antibody has been reported to be higher in infertile women (15–53%) compared with those in healthy women with normal fertility (1–3%) [317]. However, the prevalence of anticardiolipin antibody was rather low in our study (3.2%). This was contrast in another report from Korea, in which anticardiolipin antibody was positive in 14.8% among women undergoing IVF [19].
In women with unexplained infertility undergoing IVF, the prevalence of anti-β2-glycoprotein 1 antibody was 13.3% [20]. The prevalence of positive anti-β2-glycoprotein 1 antibody has been reported to be 9% in the IVF failure group, 16% in the recurrent miscarriage group, and 0% in fertile control group [21]. In our study, the prevalence of anti-β2-glycoprotein 1 antibody in women destined to the first IVF cycle was rather low (1.8%).
In the present study, clinical pregnancy rate and miscarriage rate were all similar between APA-positive and APA-negative group. These findings were consistent with most previous studies, as listed in Table 1. Thus, the screening of APA positivity appears to be unnecessary in couples who try first IVF cycle.
Currently, only 2 studies described a detrimental effect of APA on IVF outcomes. In one report from Korea, abortion rate after IVF was significantly higher in APA-positive group (62.5% vs. 20.0%), although pregnancy rate was similar between APA-positive and APA-negative group [14]. Zhong et al. [17] demonstrated a significantly lower pregnancy rate (31.3% vs. 48.6%) and higher pregnancy loss (32.0% vs. 15.1%) after IVF in anticardiolipin antibody positive women than anticardiolipin antibody negative women.
Detrimental impact of APA on miscarriage can be explained by attachment of APA to the surface phospholipids on trophoblasts. This action may cause direct cellular injury and inhibition of conversion from cytotrophoblast to syncytiotrophoblast [22]. Indirect damage on trophoblasts is also possible via formation of intravascular micro-thrombosis [323].
If APA-positive women have poorer IVF outcome, immunotherapy should be considered in APA-positive women prior to IVF. However, there is a controversy about this. A retrospective study was performed in 116 infertile women who are positive for anticardiolipin antibody; they were treated by methylprednisolone plus low-dose aspirin or not [24]. Pregnancy rate after IVF was 46.6% in treated group, 33.3% in untreated group, and 53.9% in antibody negative group. Although pregnancy rates were similar between treated and untreated group, pregnancy rate in untreated group was significantly lower than antibody negative group. However, this study included small sample size and was not a randomized study. In one small study performed in Korea, short term corticosteroid therapy has no impact on pregnancy rate after IVF [14]. Further well-designed prospective randomized studies should be conducted to verify the effectiveness of immunotherapy in APA-positive women.
Our study has several strengths and limitations. APA was measured in women scheduled for the first IVF cycle and the association of pregnancy results was prospectively analyzed. In a previous report, a higher prevalence of antiphospholipid antibodies was found in the repeated IVF failure group than control group [21], thus inclusion of women who received several IVF cycles would enhance the prevalence of antiphospholipid antibodies and this would mislead the real prevalence of APA positivity and the association between APA positivity and IVF pregnancy results.
In our study, male factor or uterine factor infertility was completely excluded. Severe form of male or uterine factor infertility would result in high miscarriage rate. In addition, we excluded women with past or current endocrine or immunologic disorders, because the presence of endocrine or immunologic disorders and treatment of those diseases could affect APA positivity.
Small sample size in APA-positive group might be a major limitation in our study. Before initiation of study, the sample size was calculated as 220 at 80% power and 5% significance level with the assumption of 20% prevalence of APA and 20% difference in pregnancy rate. However, the prevalence of APA was unexpectedly low; APA was positive in only 12 out of 193 women entering embryo transfer (6.2%). Thus, more women would be needed to assess the real association between APA positivity and IVF pregnancy results. Further adequately powered and large-scaled prospective study would be needed.
We measured only 3 APAs among various APAs and this could result in underestimation of real APA prevalence. However, it may be impractical to measure all the APA and APA not included in current classification criteria for antiphospholipid syndrome has little clinical significance [1].
In conclusion, the prevalence of APA is low in Korean infertile women undergoing the first IVF cycle and the presence of APA appears to neither decrease their first IVF success nor increase abortion rate. Thus, the screening of APA positivity appears to be unnecessary in women who try first IVF cycle.
 XML Download
XML Download