

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Embryo cryopreservation and subsequent frozen-thawed embryo transfer (FTET) are cost-effective and safe treatment to increase the cumulative pregnancy rate (PR) per oocyte retrieval. Moreover, the recent tendency toward decreasing the number of embryos transferred for prevention of multiple pregnancy highlights the importance of FTET. A variety of protocols for FTET have been developed and it has been commonly performed in natural cycles and in estrogen and progesterone replacement cycles with or without prior pituitary down-regulation [1]. Especially in patients with ovulatory cycles, natural cycle FTET is becoming an increasingly common protocol. The major advantages of FTET in a natural ovulatory cycle is that an additional hormonal therapy is not required by using the natural physiologic changes for endometrial preparation.
For a successful FTET, frozen-thawed embryo should be transferred during the implantation window of endometrium and developmental stage of embryo transferred should be synchronized with endometrial development. Therefore, it is very important to determine the optimal timing of embryo transfer (ET) in FTET cycles. Especially in natural cycle FTET, accurate time of ovulation should be ascertained in order to determine the optimal timing of embryo thawing and transfer. Therefore, serial ultrasonographic monitoring of follicular development and/or urinary luteinizing hormone (LH) test should be performed and it commonly requires many hospital visits even in women with regular cycles. Nevertheless, it is not easy to determine the exact time of ovulation, because the time interval between the onset of LH rise and ovulation varies from 24 to 56 hours and follicular mean diameter in ovulatory time is also not fixed. Therefore, administration of human chorionic gonadotropin (HCG) has become popular method for scheduling the embryo thawing and transfer in natural FTET cycles. HCG administration leads to ovulation within 36–48 hours. This trial makes ET clinically predictable and easily planned by simplifying the ovulation monitoring process. On the other hand, HCG administration can carry the risk of oocyte release from an immature follicle or luteinized unruptured follicle [2]. So far, it still remains unclear whether HCG injection for triggering ovulation affects the pregnancy outcome in natural cycle FTET. Therefore, we performed a retrospective cohort study to compare HCG-administered natural cycle with spontaneous ovulatory cycle in patients undergoing natural cycle FTET.
Materials and methods
This retrospective cohort study included 166 consecutive patients who underwent FTET in either the natural cycle after ovulation triggering with HCG (HCG group, n=110) or the natural cycle after the detection of spontaneous ovulation (control group, n=56) between January 2009 and November 2013. If patients underwent 2 or more cycles of FTET during the study period, charts corresponding to only the 1st FTET cycle were reviewed for the present study. The Institutional Review Board of the University of Ulsan College of Medicine, Asan Medical Center, approved the study (approval number: 2014-0832).
All women were between 20 and 41 years of age, and they had regular ovulatory cycles of 24–35 days in length and body mass index (BMI) between 18 and 25 kg/m2. Patients were excluded from this study if they were found to have any endocrine and metabolic disorders such as diabetes mellitus and any significant pelvic pathology such as hydrosalpinx, uterine anomaly, or fibroids with uterine cavity distortion. Subjects who had any abnormalities that would interfere with adequate stimulation or a history of previous (within 12 months) or current abuse of alcohol or drugs or a history of repeated pregnancy loss were also excluded. All women had previously undergone either conventional in vitro fertilization (IVF) or intracytoplasmic sperm injection with cryopreservation of supernumerary embryos. In all patients, cycle monitoring was started on cycle day 7 or 8 by transvaginal ultrasonography (ProSound SSD-5500; ALOKA, Tokyo, Japan) and repeated according to the size of the dominant follicle. In the HCG group, 250 μg recombinant HCG (rHCG; Ovidrel; Merck Serono SA, Geneva, Switzerland) was administered subcutaneously for triggering ovulation, when a mean diameter of the lead follicle reached 18 mm and LH surge was not detected in urinary LH test. In patients with positive result of urinary LH test on the day when the lead follicle diameter reached 18 mm, rHCG was not given and daily ultrasonographic follicular monitoring was performed for detecting a spontaneous ovulation. In the control group, serial ultrasonographic follicular monitoring was performed until ovulation was verified. Ovulation detection was documented by disappearance or typical change in the shape of the dominant follicle. The day of ovulation in the spontaneous ovulatory cycle was considered to correspond to the day of oocyte retrieval in the IVF cycle. Therefore, cryopreserved zygotes at the 2 pronuclear (PN) stage were thawed on the next day of ovulation and cultured. ET was performed 3 days after ovulation. In the HCG group, cryopreserved zygotes at the 2 PN stage were thawed on the 3rd day after rHCG injection and cultured. ET was performed 5 days after rHCG injection. Zygotes at 2 PN stage were scored according to distribution and size of nucleoli within each nucleus based on zygote grading system by Scott et al. [3].
We excluded the FTET cycles in which cryopreserved embryos at the cleaved or blastocyst stage were thawed and transferred from this study. On the day of ET, transvaginal color Doppler analysis was performed to assess the resistance index of the uterine arteries. One to 3 embryos were transferred into the uterine cavity. In all subjects, luteal support was provided by administering 90 mg of vaginal progesterone gel (Crinone gel 8%; Merck Serono SA) once daily from the 2nd day after hCG injection in the HCG group and from the ovulation day in the control group. Luteal support was continued at least up to the day of serum β-hCG measurement for pregnancy test. Serum β-hCG levels were measured by radioimmunoassay using a hCG MAIA clone kit (Serono Diagnostics, Woking, UK) with interassay and intraassay variances of <10% and 5%, respectively,11 days after ET. Clinical pregnancy was defined as the presence of a gestational sac by ultrasonography, while miscarriage rate per clinical pregnancy was defined as the proportion of patients who failed to continue development before 20 weeks of gestation in all clinical pregnancies.
Mean values were expressed as mean±standard deviation. Student's t-test was used to compare mean values. Chi-square test and Fisher's exact test were used to compare fraction. Statistical significance was defined as P<0.050. All analyses were performed by using SPSS statistical package for Windows, version 12.0 (SPSS Inc, Chicago, IL, USA).
Results
Patient's characteristics are shown in Table 1. There are no statistically significant differences with respect to age, duration of infertility, BMI, anti-Müllerian hormone level, etiology of infertility, and the number of previous IVF attempts between the 2 groups. Table 2 shows characteristics of previous fresh IVF cycle in both groups. The 2 groups were comparable with respect to the characteristics of the IVF cycle in which embryos were cryopreserved including the numbers of oocytes retrieved, mature oocytes, fertilized oocytes, grade I or II embryos and frozen embryos. There were also no differences between the HCG and control groups in clinical pregnancy rate (CPR), embryo implantation rate, miscarriage rate, live birth rate, and multiple CPR (Table 3). However, the number of hospital visits for follicular monitoring was significantly fewer in the HCG group of 3.0±1.0 compared with the control group of 4.9±1.4 (P<0.001) (Table 3).
Table 1
Patients' characteristics
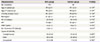
Values are means±standard deviation or number (%).
HCG, human chorionic gonadotropin; BMI, body mass index; AFC, antral follicle count; AMH, anti-Müllerian hormone; IVF, in vitro fertilization.
a)Student's t-test; b)Chi-square test or Fisher's exact test.
![]()
Table 2
Characteristics of previous fresh in vitro fertilization cycles in which embryos were cryopreserved
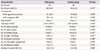
Values are means±standard deviation or number (%).
HCG, human chorionic gonadotropin; ICSI, intracytoplasmic sperm injection; COS, controlled ovarian stimulation; MDP, multiple dose protocol; rhFSH, recombinant human follicle stimulating hormone; PN, pronuclear; OHSS, ovarian hyperstimulation syndrome.
a)Chi-square test or Fisher's exact test; b)Student's t-test.
![]()
Table 3
Characteristics of frozen-thawed embyo transfer cycles and pregnancy outcome

Values are means±standard deviation.
HCG, human chorionic gonadotropin; UA, uterine arteries; ET, embryo transfer; PN, pronuclear; PR, pregnancy rate; NS = not significant
a)Student's t-test; b)Chi-square test or Fisher's exact test.
![]()
Discussion
Nowadays FTET has become a routine and integral practice in IVF treatment. FTET has been successfully performed in natural cycles following spontaneous ovulation and in cycles in which the endometrium is artificially prepared with exogenous steroids with or without pituitary suppression [4]. There is still no conclusion to show superiority of one intervention to another [5]. As the natural cycle protocol is relatively simple and reduces medication, it is preferred by many physicians and patients.
A crucial factor for embryonic implantation in FTET is synchronization between embryonic and endometrial development. Therefore, preparation of endometrium having receptivity and the timing of ET is very important in FTET cycles. The timing of events that lead to endometrial receptivity might be associated with the type of signal triggering ovulation. Apparently, in the presence of the LH surge, the cascade of events leading to ovulation and a receptive endometrium is initiated naturally and driven primarily by the LH surge itself and to a lesser extent by exogenous HCG. However, the problem of natural cycle FTET is the timing of ET. The decision of ET is decided by accurate ovulation detection. For the accurate determination of ovulation, the patients should be monitored with serial ultrasonographic examination of ovarian follicles and/or hormonal assays. Nevertheless, it is difficult to determine the exact time of ovulation and therefore natural FTET cycles is cancelled in approximately 6% [6]. Because of the above problems, ovulation triggering by HCG has introduced and recently performed widely. HCG induces ovulation and also may affect early embryonic development and implantation. Implantation and ongoing pregnancy depend on a synchronized dialogue between a receptive endometrium and embryo. Although many studies on the HCG effect on endometrium have been performed, there is disagreement about advantage or disadvantage of HCG administration. Kyrou et al. [7] reported higher ongoing PR in patient group with spontaneous LH surge compared with HCG-administered group in patients undergoing natural cycle intrauterine insemination. The reason might be explained that ovulation and implantation are driven primarily by the LH surge itself and to a lesser extent of exogeneous HCG [8]. LH has a role of major paracrine regulator and induces meiosis resumption of oocyte. If exogenous HCG might be given earlier before LH surge, exogenous HCG may release an oocyte from immature follicles. On the contrary, Mansour et al. [9] reported that HCG increases endometrial progesterone receptors and its level is positively correlated with the level of trophoblastic tolerance. Weissman et al. [10] reported that there are no differences in terms of FTET outcome between the spontaneous ovulatory cycle group and HCG administration group in FTET.
As described above, studies on the effect of exogenous HCG on pregnancy outcome have shown inconsistent results. Nevertheless, dose-finding study to determine an optimal HCG concentration for natural cycle FTET has not been reported yet. Therefore, well-designed large studies on exogenous HCG administration in natural cycle FTET are needed. The present study showed no significant differences in FTET outcome between the HCG-administered group and spontaneous ovulatory cycle. However, the number of hospital visits for follicular monitoring was significantly lower in the HCG group than in the spontaneous ovulatory cycle group. The fewer hospital visits make the treatment process simple and reduce the medical cost, physician's workload and patient's inconvenience.
In this study, HCG administration for ovulation triggering reduced the number of hospital visits without adverse effect on cycle outcome. These results suggest that HCG-administered natural cycle is feasible, effective and patient friendly protocol for FTET in patients with spontaneous ovulation.
 XML Download
XML Download