

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Benign multicystic peritoneal mesothelioma (BMPM) is a rare tumor that occurs frequently in women of reproductive age with a previous history of abdominal surgery. Multicystic peritoneal mesothelioma was first described in 1979 by Mennemeyer and Smith, and since then approximately 150 cases have been described in the literature [1]; however, cases managed by laparoendoscopic single site surgery (LESS) are rare [2]. The pathogenesis of this condition remains unclear but it is likely the result of a chronic inflammatory process, as in the case of endometriosis [3]. Diagnosis before surgery and the differential diagnosis of an ovarian tumor are difficult. The treatment of choice is complete surgical excision. The rate of recurrence is high and malignant transformation is possible. We report a rare case of BMPM presenting as small multilocular cystic mass in the pelvic cavity with abdominal pain in a menopausal woman, which was treated with single port laparoscopy.
Case report
This case was approved by the Institutional Review Board of Daejeon St. Mary's Hospital, The Catholic University of Korea College of Medicine (DC16 ZISE0032).
A 47-year-old woman, gravida 3, para 1 had a 2-day history of low abdominal pain. The pain was intermittent and dominant on the left side. Her vital signs were normal. She experienced menopause 5 months ago. Past medical history was unremarkable. She had a history of previous gynecologic surgery at local hospital in 2010. The surgery performed was right ovary cystectomy with adhesiolysis by laparotomy. Pathology indicated right ovarian mucinous cystadenoma. Familial history was not notable.
On physical examination, the abdomen was mildly distended. Pap smear test results were within normal limits, and laboratory findings were within normal range. Cancer antigen (CA)-125 level was slightly elevated at 60.55 (reference range, 0–39 U/mL) and CA19-9 level was 5.510 (reference range, 0–35 U/mL). Estradiol (E2) level was <5 (reference range, menopause: under 10 pg/mL) and follicle-stimulating hormone level was 55.82 (reference range, menopause: 25–134 mIU/mL). Ultrasonography (Fig. 1A) and computed tomography (CT) of the pelvis revealed a multilocular cystic mass in the pelvic cavity. CT findings indicated that pseudomyxoma peritonei could be ruled out because of loculated fluid collection in both the paracolic gutters and multiple low dense cystic lesions in the omentum and mesentery. Magnetic resonance imaging (MRI) revealed small multiple nodules about 1 cm in size with low signal intensity in the anterior and posterior uterine wall on T2-weighted images and multiple nodules with 4.6 cm and 2.8 cm sized heterogeneous signal intensity in the pelvic cavity on T1-weighted images (Fig. 1B).
Fig. 1
(A) Ultrasonography of the pelvis shows a multilocular cystic mass in the pelvic cavity. (B) Magnetic resonance imaging shows small multiple nodules about 1 cm in size with low signal intensity in the anterior and posterior uterine wall on T2-weighted images.

We decided to perform laparoscopic surgery. A laparoscopic trocar was placed in the umbilicus. During laparoscopy, we observed multiple grapelike clusters of cysts within the pelvic cavity (Fig. 2A). The cysts appeared to originate from the peritoneum and attached to the uterus and both adnexa (Fig. 2B). Additional small cysts were found on the omentum, small bowel mesentery, and appendix (Fig. 2C). Intraoperative frozen section histology of the multiple grapelike clusters of cysts indicated possible mucinous-type benign cysts. Excision of all macroscopic visible cysts was selected as the treatment procedure. Excision of multiple clusters of cysts in the pelvic cavity, resection of the uterus with both adnexa, appendectomy, omentectomy, and adhesiolysis were performed.
Fig. 2
(A) On laparoscopy, multiple grapelike clusters of cysts appear to originate from the peritoneum. (B) multiple cysts are attached to the uterus and both adnexa. (C) Additional small cysts are seen on the omentum, small bowel mesentery, and appendix. (D) Calretinin immunohistochemical staining (×100) reveals a positive reaction.
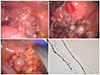
Grossly, the right ovarian cyst measured about 2×2 cm in size. Microscopically, the cysts were multiple thin-walled translucent small cysts with clear fluid. The lining cells were immunohistochemically reactive for pan-cytokeratin and calretinin (Fig. 2D). Histological examination findings of the excised specimens were consistent with benign multicystic mesothelioma of the pelvic peritoneum. The postoperative course was uneventful. The patient is well for 2 years with no clinical evidence of disease recurrence.
Discussion
BMPM is an uncommon tumor that originates from mesothelial cells. The diagnosis of this disease before surgery and differential diagnosis are difficult. Differential diagnosis includes lymphangioma, pseudomyxoma peritonei, malignant peritoneal mesothelioma, and cystic adenomatoid tumor [4]. BMPM occurs most frequently in women of reproductive age. Cases of BMPM in men have been reported, although very rarely. A report on the analysis of 37 patients with BMPM showed that 83.8% of the patients were female and their average age was 38 years. As the disease is found in 37.8% of subjects in their 50s, in 5.3% of subjects in their 60s and in 10.8% of subjects in their 70s, as well as in infants, it is suggested that BMPM may occur in patients at all ages [5].
The most common presenting symptoms are intermittent abdominal pain, tenderness or distention, and a palpable mass. The etiology of BMPM is controversial but is probably neoplastic or reactive. BMPM is reported to be neoplastic because it can progress to the malignant form, and reactive in women because of the strong association with surgical intervention, inflammatory disease, or endometriosis [6]. Unlike pleural mesothelioma, BMPM is not associated with prior exposure to asbestos like in our patient.
BMPM manifests as grapelike, multilocular, thin-walled cysts containing translucent fluid and multiseptated anechoic cysts on ultrasonography. CT and MRI findings confirm ultrasonographic findings but do not permit differentiation from other cystic lesions. On MRI, BMPM exhibits low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, reflecting high fluid content [7].
In our case, initial CT could not distinguish pseudomyxoma peritonei from BMPM. Intraoperative frozen section histology indicated a benign condition. Pathology confirmed diagnosis. Immunohistochemistry showed positivity for calretinin. Therefore, the disease was diagnosed as BMPM.
Laparoscopy remains the best diagnostic tool because it enables to perform biopsies and to establish the definitive diagnosis [8]. There are no evidence-based treatment strategies for BMPM. Complete surgical excision to prevent recurrence and possible malignant transformation remains as the treatment of choice. More aggressive approaches such as cytoreductive surgery with standard peritonectomy procedures in combination with hyperthermic intraperitoneal chemotherapy (HIPEC) have been recently proposed [910]. Some studies suggest that cytoreductive surgery and HIPEC can provide better disease control than debulking surgery alone, considering the high risk of recurrence and the possibility of malignant transformation in a patient inadequately treated. But, there is still insufficient to be considered as the first treatment for these procedures. In addition, hormonal therapy with anti-estrogens and gonadotropin-releasing analogues has been attempted. Adjuvant chemotherapy and radiotherapy are not indicated, as this tumor has a prevailing benign character. Malignant transformation is extremely rare, with 2 cases reported [11]. Careful long-term follow up is important because of the high rate of recurrence (27%–75%).
LESS has been used for surgery of various benign disease and early stage cancers in the gynecologic field [1213]. In recent meta-analyses comparing LESS and multiport laparoscopy during gynecologic surgery [14], it was determined that LESS involves longer operative times and better cosmetic result with similar outcomes.
We have used LESS as the first-line procedure for ovarian masses since 2011 in our hospital. In some cases, we converted to additional port laparoscopy or laparotomy after initial biopsy. LESS is cosmetically appealing because only one wound is involved and the mass can be easily removed because of the relatively large umbilical incision site [15]. In this case, analysis of the frozen section of the ovary cyst and multicystic mass indicated a benign nature, so the mass was completely removed by LESS and the patient didn't recur for 2 years until now.
In conclusion, preoperative diagnosis of BMPM is difficult. This disease should be considered when grapelike multicystic structures are seen on ultrasonography. Differential diagnosis should include other malignant lesions is needed. Malignant transformation of BMPM is extremely rare, but the recurrence rate of this disease can be up to 50%. Therefore, careful follow up is recommended.
 XML Download
XML Download