

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Coronary arteriovenous fistula (CAVF) is defined as an abnormal fistulous connection between a coronary artery and any of the 4 chambers. This condition is rare, accounting for 0.002% of the general population [1]. The most common type of CAVF is a fistulous communication between the coronary artery and cardiac chambers (75%), followed by the pulmonary artery (17%), coronary sinus (7%), and superior vena cava (1%) [1]. Prenatal diagnosis of CAVF has been reported since 1996 [2], and a majority of the prenatally diagnosed CAVFs are associated with outflow tract obstructive lesions with an intact ventricular septum, such as pulmonary atresia and hypoplastic left heart syndrome [23]. However, few cases of isolated CAVF have been reported to date. We successfully diagnosed the fistula between the left coronary artery and coronary sinus by prenatal echocardiography. To the best of our knowledge, this is the first report of a prenatally diagnosed fistula between the left coronary artery and coronary sinus.
Case report
A 23-year-old woman, gravida 1, para 0, was referred to our institution for a detailed cardiovascular evaluation for hypoplastic left heart syndrome at 25.3 weeks of gestation. Her medical and family histories were unremarkable. Initial fetal echocardiography demonstrated situs solitus with atrioventricular and ventricular arterial concordance. A 4-chamber view of the heart revealed mild dilatation of the right atrium and right ventricle without tricuspid regurgitation. In the 5-chamber view, the left coronary artery was dilated and directly connected to the coronary sinus (Fig. 1A). Power Doppler sonography confirmed the presence of the fistula between the left coronary artery and coronary sinus (Fig. 1B); thus, the diagnosis of a CAVF was made. A relatively small aorta was observed after branching of the left coronary artery without any obstruction signs, and color Doppler showed reversal flows in the ascending aorta and aortic arch during the diastolic phase. No other abnormalities were detected, and the parent refused fetal karyotyping.
Fig. 1
The 5-chamber view of the heart at 25.3 weeks showing the fistula between the left coronary artery and coronary sinus (arrow, A). Power Doppler imaging confirming the communication between the left coronary artery and coronary sinus (B). The 4-chamber view of the heart at 29.6 weeks showing the dilated coronary sinus (arrow) with the collapsed left atrium (C).
Ao, aorta; CS, coronary sinus; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.

Follow-up echocardiography at 29.3, 33.5, and 36.5 weeks of gestation revealed that the CAVF was more obvious and the coronary sinus had become dilated, inducing compression of the left atrium (Fig. 1C). There were no signs of cardiac impairment during the prenatal period. A female neonate was born at 39.4 weeks of gestation. The birth weight was 3.24 kg and the Apgar scores were 9 and 9 at 1 and 5 minutes, respectively.
Immediately after delivery, the neonate was stable with a heart rate of 170 bpm, and oxygen saturation of 100% at room air. Postnatal echocardiography and cardiac computed tomography showed the dilated left main coronary and left circumflex arteries with a fistulous connection to the severely dilated coronary sinus (Fig. 2). The aorta was unobstructed, with no evidence of coarctation of aorta. Electrocardiography showed ST changes in the whole precordial leads, suggesting myocardial ischemia, and cardiac catheterization was performed for a trial of catheter intervention. Angiography also showed findings similar to those of the postnatal echocardiography. However, catheter intervention could not be performed because of a very large fistula tract. On the third day of life, the neonate underwent surgical repair for CAVF coupled with ligation of the ductus arteriosus and closure of the atrial septal defect. Subglottic stenosis occurred postoperatively and was successfully treated by laser dissection. She was discharged after 2 months of hospitalization. Currently, at the age of 1 year, the baby is doing well without any complications.
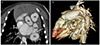
Fig. 2
Postnatal computed tomography showing the dilated left circumflex artery draining into the enlarged coronary sinus on the axial image (arrow, A) and the 3-dimensional volume rendering image (arrow, B).
Ao, aorta; CS, coronary sinus; LAA, left atrial appendage; LCX, left circumflex coronary artery; LMA, left main coronary artery; PA, pulmonary artery.
Discussion
To the best of our knowledge, this is the first report of a fistula between the left coronary artery and coronary sinus successfully diagnosed by prenatal echocardiography. To date, few cases of isolated CAVF have been diagnosed prenatally [4567891011]. All isolated CAVFs that were diagnosed prenatally drained into the cardiac chambers, and there were no cases with connections to the vascular structures rather than the cardiac chambers, such as the pulmonary artery, coronary sinus, and superior vena cava. In our case, prenatal ultrasonography was sensitive enough to diagnose CAVF draining into the coronary sinus.
Although the normal coronary artery is usually difficult to visualize prenatally because of the small size of the vessel, coronary malformations, such as CAVF, can be diagnosed with a high accuracy by fetal echocardiography. In this case, we clearly demonstrated the fistulous tract connected to the dilated coronary sinus. When the echocardiographic findings, such as cardiomegaly, dilated coronary artery, and abnormal jet flow into the cardiac chambers or great vessels that the CAVF enters, are obtained prenatally, a CAVF should be suspected [9]. We also observed reversal flows in the ascending aorta and aortic arch, and these findings were considered to be a coronary “steal phenomenon” because of the runoff of blood from the high-pressure coronary arteries to a low-resistance draining cavity [12].
Most infants with CAVF are generally asymptomatic. However, a majority of the patients with prenatally diagnosed CAVFs showed symptoms related to congestive heart failure; therefore, they underwent closure of the fistula. There was only one case of spontaneous closure of a prenatally diagnosed CAVF. Based on these findings, it is speculated that patients with prenatally diagnosed CAVFs are more likely to experience congestive heart failure than those of with postnatally diagnosed fistulas. CAVF may cause heart failure during the prenatal period, resulting in fetal hydrops. Two cases of CAVF associated with fetal hydrops were reported, and both neonates died on the day of delivery [78].
Symptomatic patients should be treated by either percutaneous or surgical closure. Surgical closure is generally accepted in cases of large symptomatic fistulas or fistulas complicated by other cardiac defects [13]. In our case, the retrograde flow in the ascending aorta detected by prenatal and postnatal echocardiography and widespread ST changes on electrocardiography suggested a significant steal phenomenon, and progressive elevated B-type natriuretic peptide suggested a large shunt flow from the fistula and the patent ductus arteriosus. These findings indicated early surgical correction. The neonate in this case underwent a surgical correction on the third day after birth without any complications. The prenatal detection of CAVF is of importance for the appropriate treatment and prevention of complications.
In conclusion, we reported an extremely rare case of abnormal vascular connections involving the left circumflex coronary artery and coronary sinus. A careful echocardiographic examination in the prenatal period is applicable for the diagnosis of a CAVF and aids its timely management.
 XML Download
XML Download