

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Approximately 10% of women under age 40 have elevated serum follicle stimulating hormone (FSH) level which does not correspond to the strict definition of premature ovarian failure [12]. Diminished ovarian reserve (DOR) per se can cause female infertility even though they are young and it is commonly encountered in in vitro fertilization (IVF) clinics [3]. In our center, DOR was identified in 15.3% (when a cutoff of serum anti-Müllerian hormone [AMH] was <0.76 ng/mL) and 26.1% (when a cutoff of serum AMH was <1.1 ng/mL) among 176 women participating IVF [4]. Recently ‘expected DOR’ was proposed by the Bologna criteria, defined by (1) below the age of 40 years and/or previous ovarian surgery, and (2) an abnormal ovarian reserve test (AMH <0.5–1.1 ng/mL or antral follicle count [AFC] <5–7) [5]. The causes of DOR are largely unknown, although some women have a history of ovarian surgery, chemotherapy, pelvic irradiation, or rarely associated with genetic or autoimmune disease [3].
Although there is still ongoing debate on how to manage endometriomas before IVF, a Cochrane review suggested that surgery of endometriomas before IVF has no beneficial effect on the reproductive outcomes [6]. It is well known that ovarian reserve is commonly decreased after surgical treatment of endometrioma [26789]. Therefore, before undergoing surgery, clinicians should counsel women regarding the risks of decrease of ovarian reserve. Several studies have reported a poor response to ovarian stimulation and a significantly impaired IVF outcome in women who underwent endometrioma cystectomy compared with women with tubal factor infertility or endometriosis without previous cystectomy [7891011121314]. A previous study reported that fewer number of follicles were recruited and fewer oocytes collected from the patients who had had endometrioma removed compared with those who had had simple cysts removed [10].
These results have suggested that, in the case of endometrioma operation, the reason for poor IVF outcome is mainly caused by DOR. Therefore, it is thought that if the patient does not have DOR after endometrioma operation, she would have good IVF outcome. However there are few studies compared IVF outcome among the patients with surgery-induced DOR. Furthermore studies for IVF outcome according to the etiology of DOR are rarely found.
The aim of this study was to compare the IVF outcomes between women with DOR after endometrioma operation and women with DOR without ovarian surgery.
Materials and methods
A retrospective study was conducted in women aged under 40 who underwent fresh IVF cycles between March 2010 and December 2015. Their first and second IVF cycles were included. DOR was defined by serum AMH <1.1 ng/mL or AFC ≤6.
The group of DOR after endometrioma operation included women with DOR who had a history of surgery for the endometrioma (unilateral and bilateral cystectomy, or unilateral oophorectomy), regardless of current presence of endometrioma at the time of IVF. The second group, DOR without ovarian surgery, included women with DOR who had no history of ovarian surgery, systemic chemotherapy, or pelvic irradiation; in this category, women with current benign cysts were included but women with current endometrioma were excluded. Two patients of pelvic endometriosis without surgery were included in DOR group without ovarian surgery. Most of the uterine factors consisted of myomas and endometrial polyps, in addition uterine factors included two cases of endometrial cancer and one case of thin endometrium.
Patients underwent IVF with fresh embryo transfer. Two types of pituitary suppression protocol were used: luteal long protocol (35 cycles) (gonadotropin releasing hormone agonist administration in the luteal phase of the previous cycle) or antagonist protocol (109 cycles) (daily gonadotropin releasing hormone antagonist administration from stimulation day 6). In 23 cycles, no pituitary suppression was applied. Recombinant or urinary FSH with or without luteinizing hormone was variably used but the IVF outcomes were not separately analyzed according to the regimen of ovarian stimulation.
After two or more follicles had reached a diameter >18 mm, 250 µg of recombinant human chorionic gonadotropin (Ovidrel, Merk-Serono, Geneva, Switzerland) was injected. The oocyte was retrieved 35 hours after the human chorionic gonadotropin injection. The number of mature oocytes was calculated as the summation of the second meiotic metaphase oocytes and the first meiotic metaphase-derived second meiotic metaphase oocytes. Fertilization rate was calculated as the number of zygotes with two distinct pronucli and a second polar body divided by the number of mature oocytes. The quality of embryos was evaluated by morphological criteria based on the fragmentation degree and the regularity of blastomeres on day 3 after fertilization and classified as four grades (with grade A being the top embryos). We assess blastocyst quality method present by Gardner et al. [15].
Embryo transfer was performed day 3 to 5 after the oocyte collection. Luteal phase was supported either by daily progesterone injection or vaginal gel (Crinone, Merck Serono). Pregnancies were diagnosed by positive urinary human chorionic gonadotropin test 14 days after oocyte collection. Clinical pregnancies were confirmed by the presence of a gestational sac on vaginal ultrasound examination during the 5th week.
In the present study, the primary end-point was the live birth rate. Secondary end-points were cycle cancellation rate (due to poor response or total fertilization failure), number of retrieved oocytes, number of mature oocytes, fertilization rate, clinical pregnancy rate, and spontaneous abortion rate. All statistical analyses were performed using IBM SPSS ver. 19 (IBM Corp., Armonk, NY, USA). The data were analyzed using the Mann-Whitney U-test or Fisher's exact test as indicated. The results were considered significantly different when the P-value was <0.05.
Results
We enrolled 124 women (166 cycles) with DOR and divided them into two groups; the group of DOR after endometrioma operation (n=32, 47 cycles) and the group of DOR without ovarian surgery (n=92, 119 cycles).
Clinical and laboratory characteristic are shown in Table 1. There were significant differences in patients' age and the husbands' age between two groups. The surgery-induced DOR group was younger than the DOR group without ovarian surgery (34 [33–35] vs. 36 [35–37], P<0.001). Other characteristics were similar in both groups.
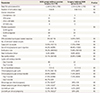
The data regarding the controlled ovarian stimulation and IVF cycle outcomes are shown in Table 2. AFC, AMH, total dose of gonadotropin and the duration of ovarian stimulation were not different in two groups. Cycle cancellation rate, fertilization rate, number of retrieved mature oocytes and top quality of embryo were similar rate in both two groups.
Clinical pregnancy (per transfer, 17.4% vs. 28.9%; per cycle, 8.5% vs. 20.2%) and live birth (per clinical pregnancy, 50% vs. 72.7%; per cycle, 4.2% vs. 13.4%) tend to be lower in the surgery-induced DOR group compared with DOR without ovarian surgery, but there were not different statistical significances.
Discussion
In this study, we observed IVF outcomes of patients with DOR after endometrioma operation compared with group of DOR without ovarian surgery. In the similar range of AMH and AFC in both groups, there are no differences of IVF outcomes significantly.
Previously, there were severe studies comparing IVF outcomes between group of endometriosis operation and tubal infertility. The most studies approved high cancellation of IVF cycles or higher dose of FSH in group of endometriosis operation compared with tubal infertility group. It is thought that there was DOR after endometriosis operation, so its result decreased ovarian response. However, it failed to find consensus regarding pregnancy rate and live birth rate [7811121316].
A previous study of IVF outcomes following etiology of DOR demonstrated that group of DOR after endometrioma cystectomy resulted in lower rate of fertilization, top quality embryo (8.2% vs. 13.0%, P=0.046), clinical pregnancy (11.2% vs. 20.6%, P=0.02) and live birth (7.2% vs. 16.9%, P=0.02) compared with group of idiopathic DOR [17]. In the study, they suggested the mechanisms of inferior IVF outcomes in the group of endometriosis operation were lower quality embryo and endometrial receptivity.
However, in our study, all parameters of IVF outcomes were not significantly different in the group of endometrioma operation compared with DOR without ovarian surgery. Especially pregnancy rate and live birth rate were not different whatever etiology of DOR Age variable is different significantly, so we adjusted age variable, and it resulted same as above.
Except cycle cancellation patients, we observed similar range of mean number of mature oocytes retrieved in both groups. Furthermore similar rate of top quality embryos and fertility rate were shown. It is thought that endometriosis is not detrimental effect for oocyte quality and embryo quality in same condition of DOR.
Our strength compared with the previous study is that we studied only the 1st and 2nd cycles of IVF, because biases can increase when several IVF cycles per patient were included in study. However, the sample size was relatively small and and our study provided statistically insignificant evidence that the chances of IVF success are decreased in women with DOR after endometrioma operation. Further study of larger series is needed to confirm these findings. Another limitation is that data were collected retrospectively using the database of our department. However, this study is not appropriate for randomized controlled trial. There are many debates for treatments of endoemtrioma before IVF. For making proper treatment of endometrioma before IVF, more randomized controlled trials are needed comparing IVF outcomes between expectant management and surgical management of endometrioma.
In conclusion, we found that ovarian stimulation and IVF cycle outcomes including clinical pregnancy and live birth rate were not different significantly whatever etiology of DOR. We suggest that the most important factor of endometriosis related infertility is DOR, not reduced endometrial receptivity and inferior oocyte and embryo quality.

 XML Download
XML Download