

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Carcinoid tumors are a slow-growing type of neuroendocrine tumors. Neuroendocrine tumors originate mainly from gastroenteric tissue, pancreatic islet cells, neuroendocrine cells within the respiratory epithelium, and parafollicular cells distributed within the thyroid. They occasionally have secretory characteristics, and the patients present with a rather unusual and complex disease spectrum with various conditions, such as flushing, diarrhea, hirsutism, or constipation [12].
Primary carcinoid tumors of the ovary account for <0.1% of all ovarian malignancies and only 5% of carcinoid tumors are of the ovarian origin [2]. There are 4 subtypes in primary ovarian carcinoid tumors: insular, trabecular, mucinous, and strumal. The insular type is the most common and is associated with the typical carcinoid syndrome caused by serotonin and its precursors. The trabecular carcinoid is a rare, slow-growing tumor that has not been associated with carcinoid syndromes. Mucinous carcinoids are typically more aggressive manner than other types. In contrast, the strumal type is the least common and is characterized by a mixture of thyroid and carcinoid tissues [1]. Most tumors are either seen in perimenopausal or postmenopausal women with nonspecific symptoms like enlarging mass, or are found incidentally on imaging [3]. The production of peptide YY (PYY), a gastrointestinal hormone, by ovarian tumors may decrease intestinal motility. PYY is presumably the main cause of the constipation in patients with ovarian carcinoid tumor. Herein, we report a rare case of a PYY producing strumal carcinoid tumor of the ovary in a postmenopausal woman presenting with severe progressive constipation, which resolved rapidly after surgery.
Case report
A 64-year-old postmenopausal woman visited the gastroenterology clinic for persistent, severe constipation for the last 5 years; she was referred to our gynecological department because of a concurrent ovarian tumor. Recently, the symptoms had worsened to a point that she defecated only once every 7 to 10 days despite taking daily laxatives since the last 5 to 6 months. There was no remarkable past clinical history other than degenerative arthritis. Her family history was unremarkable. On abdominal examination, the upper abdomen was distended with tympanic sound and the lower abdomen was soft with audible bowel sound. Gastroduodenoscopy and colonoscopy revealed no abnormalities. Results of routine blood tests, including complete blood count, electrolyte, liver function test, renal function test, and thyroid function test, were normal. Ultrasound evaluation revealed a soild mass measuring 6.5×5.2 cm in the right ovary. Subsequent computed tomography (CT) of the abdomen and pelvis was performed to evaluate the structural cause for constipation and to rule out primary gastrointestinal tract disease. CT showed a well-defined right adnexal mass measuring 6.4 cm with hyper-enhancement relative to the uterine myometrium (Fig. 1A). Serum tumor markers, such as cancer antigen-125, human epididymis protein 4, and carcinoembryonic antigen, were within normal limits.
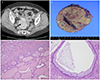 | Fig. 1(A) Contrast-enhanced computed tomography shows a well-defined hypervascular solid mass (arrow) in the right adnexa (uterus [U]). (B) On gross examination, the solid, pink-white tumor of the ovary measured 6.3×5.5×5.3 cm and had smooth outer surface and intact capsule. (C) Histopathologic examination revealing a carcinoid tumor associated with thyroid tissue (hematoxylin and eosin [H&E], ×100). (D) There are only a few glands lined by columnar epithelium with goblet cell (H&E, ×200).
|
Laparotomy revealed a smooth, solid tumor in the right ovary, and only a small amount of ascites were observed in the pelvic cavity. No abnormalities were found in the left adnexa, uterus, or abdominal cavity. Right salpingo-oophorectomy was performed. The ovarian mass did not adhere to or compress the colon. Intraoperative frozen section examination suggested a strumal carcinoid tumor with suspicious foci of papillary thyroid carcinoma. Consequently, abdominal total hysterectomy, left salpingo-oophorectomy, and omentectomy were performed. Cytological examination of the cells in the ascites was negative.
On gross examination, the tumor was predominantly solid with an intact capsule (Fig. 1B). It measured 6.4×5.5×5.3 cm and weighed 109.5 g. The cut surface revealed a pinkish-white solid mass with a few cystic areas. On histopathologic examination, trabeculae and small nests of uniform tumor cells associated with acini resembling thyroid follicles were observed. Cytologic atypia was not definite on the permanent sections. There were few intestinal-type mucinous glands with goblet cells (Fig. 1C and D). On immunohistochemical staining, the tumor cells were found to be diffusely positive for PAX8 (Fig. 2A). They were immunoreactive for synaptophysin in carcinoid areas (Fig. 2B) and for thyroglobulin in struma areas (Fig. 2C). The immunohistochemical staining for PYY was performed additionally and the result was strongly positive (Fig. 2D). The final histological examination confirmed that the mass was a strumal carcinoid tumor of the right ovary without surface involvement, corresponding with International Federation of Gynecology and Obstetrics stage IA.
 | Fig. 2Immunohistochemical staining. (A) The tumor cells are diffusely positive for PAX8. (B) Carcinoid part of the tumor shows positive immunoreactivity for synaptophysin. (C) Follicles are surrounded by cells immunohistochemically positive for thyroglobulin. (D) Most of the cytoplasm of carcinoid tumor cells is positive for peptide YY.
|
The patient recovered well in the postoperative period. At 1-month follow-up, her constipation had dramatically resolved, and she could pass stools regularly without any laxative. After 16 months of postoperative follow-up, the patient has remained well without any evidence of tumor recurrence.
Discussion
Primary carcinoid tumors of the ovary account for <0.1% of all ovarian malignancies, and only 5% of carcinoid tumors are of the ovarian origin [2]. The ovarian carcinoid tumors are typically divided into 4 categories based on the histopathologic patterns: insular, trabecular, mucinous, and strumal [3]. Strumal carcinoid tumors are an unusual subtype of ovarian carcinoid tumors and are characterized by a mixture of thyroid and carcinoid tissues [1].
The majority of patients with primary ovarian carcinoid tumors have no specific signs or symptoms, and tumors may be found incidentally on imaging. Some patients may suffer from abdominal pain, palpable mass, constipation, and hirsutism [4]. Constipation may be seen in strumal and trabecular types associated with PYY production. PYY producing carcinoid tumor is rare among primary carcinoid tumors of the ovary, and the incidence was not reported accurately.
Primary carcinoid tumor of the ovary accompanying severe constipation was first reported in 1992 [4]. Motoyama et al. [4] reported that PYY positive cells were present in more than 50% of all their recruited patients. This suggested that constipation was caused by PYY protein and not by the mechanical effect of the tumor itself [5]. PYY is a gastrointestinal polypeptide hormone comprising 36 amino acids; it is mainly present in the endocrine cells of the distal intestine, particularly of hindgut derivation. It has a strong inhibitory effect on jejunal and colonic motility [6]. To the best of our knowledge, there are no reports about the relationship between proportion of PYY expression and severity of constipation. According to the results reported so far, more than 50% of entire tumor cells showed diffuse immunohistochemistry staining with PYY in primary ovarian carcinoid tumors presenting with constipation. Therefore, we can presume that the threshold for the development of constipation is at least 50% of entire tumor cells [7].
The primary strumal carcinoid tumor is of low malignant potential and tends to be benign if it is confined to one ovary. The 10-year survival rate approaches almost 100% [8]. The standard treatment of primary ovarian carcinoid tumors is complete resection by oophorectomy or salpingo-oophorectomy. Adjuvant chemotherapy or radiotherapy is usually neither recommended nor required. Unlike primary carcinoid tumors, metastatic carcinoids are more aggressive with one-third of the patients dying within 1 year and three-fourths dying within 5 years after initial diagnosis [9]. Thus, differential diagnosis of the primary carcinoid tumor from the metastatic tumor is important.
Radiologically, the imaging appearance of ovarian carcinoid tumors is not well described due to its rarity. Primary ovarian strumal carcinoid tumor does not have characteristic imaging findings. Therefore, preoperative diagnosis of these tumors may be difficult. Because these are solid tumors, they would be indistinguishable from solid primary ovarian cancer or metastasis, although necrosis is less common in the former. Most cases have been diagnosed based on postoperative pathology findings [10].
In our case presented here, there was no adhesion to or compression of the surrounding soft tissues and the gastrointestinal tract. Moreover, the size of tumor was too small to compress other organs. After tumor removal, the patient's constipation completely resolved within a few days. Although the possibility that the effect of pelvic organ prolapse was related to the constipation cannot be excluded completely, in pelvic examination, she had mild pelvic organ prolapse (stage I) according to Pelvic Organ Prolapse Quantification system. Hence, we assert that the possibility of pelvic organ prolapse as the main cause of constipation may be low.
Gynecologic causes could have been behind the persistent constipation. For instance, hormonal imbalance, pelvic organ prolapse, fibroids, endometriosis, adenomyosis and ovarian tumors (benign or malignant) can all cause persistent constipation. Both estrogen and progesterone are associated with intestinal movement; recent studies have suggested that estrogen and not progesterone may be a detrimental factor of constipation owing to decreased bowel motility [11]. The upper posterior vaginal wall may be associated with bowel disorders, including constipation or flatal incontinence. Anatomical changes in the posterior vaginal wall are partly responsible for the symptoms [12]. The endometriosis located in adjacent areas, such as the rectovaginal septum, uterosacral ligaments, and the pouch of Douglas, can cause constipation rather than the implants on the surface of the bowel [13]. Constipation can be caused by the mass effect of ovarian cancer, the chemotherapy regimen used to treat it, or painkillers, such as opioids. Moreover, ovarian cancer patients are often more sedentary; thus, constipation in them may have exacerbated due to inactivity [14]. Therefore, when women present with persistent constipation without any gastrointestinal problem, gynecologic causes need to be considered.
This is an undiagnosed, untreated, and progressive case with protracted course. The cause of constipation was not recognized till operation. Medical treatment, lifestyle changes, and fiber rich foods were not effective to relieve the symptom.
In conclusion, the demonstration of PYY expression via immunohistochemical analysis in our case supports that PYY protein, produced by ovarian carcinoid tumor, may be associated with severe constipation by disturbing distal intestinal motility. In women who present with an ovarian mass associated with severe persistent constipation, ovarian strumal carcinoid tumor should be considered as a differential diagnosis.
 XML Download
XML Download