

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Epithelial ovarian carcinoma is the second most frequent gynecologic malignancies in the United States with the highest mortality [1]. One of the reason is that most patients are diagnosed at advanced stages usually involving distant metastases. The most common sites of distant metastases are pleura (25%), liver (9%), lung (7%), and lymph nodes (7%). Skin involvement of ovarian carcinoma is very rare. Its incidence ranges from 1.9% to 5.1% [2345]. The most common metastatic sites of skin are abdominal wall, followed by chest wall, and breast. Clinical manifestation of skin metastases may be presented as nodular lesions, carcinoma erysipeloides, or large cauliflower-like lesions that mimic erysipelas or cellulitis [26].
Skin metastases occur late in the course of the disease. They are associated with poor prognosis [7]. We present a case of skin metastases in a patient with ovarian clear cell carcinoma on chest wall. Such case is rare and difficult to diagnose with poor prognosis.
Case report
A 54-year-old menopausal woman (nulligravida) was admitted to our department complaining of abdominal distension for 5 months that was aggravated 2 months ago. The ultrasound demonstrated a 11×10×9 cm3 mass in the right adnexal region and a 13×11×8 cm3 mass in the left adnexal region with massive ascites. These masses were irregular, multilocular, solid, and cystic tumor covered with strong vascularity.
Preoperative value of cancer antigen 125 (CA-125) was at 1,247 U/mL (reference range, 0 to 35 U/mL). Magnetic resonance imaging showed ovarian tumors, omental cake, and massive ascites suggesting carcinomatosis peritonei. Positron emission tomography also indicated malignant mass in pelvic cavity with small amount pleural effusion and in left hemithorax. Abdominopelvic computed tomography (CT) revealed suspicious metastatic lymph nodes at para-aortic, aortocaval, both common iliac arteries, and left internal iliac artery. Result of ascitic fluid cytology by paracentesis was carcinoma with clear cell and papillary feature.
We performed cytoreductive surgery with total abdominal hysterectomy, bilateral salpingo-oophorectomy, bilateral pelvic lymph node dissection, para-aortic lymph node dissection, omentectomy, total pelvic peritonectomy, partial hepatectomy, diaphragm stripping with partial diaphragmectomy, splenectomy, and mesenteric tumorectomy on November 2015. Histopathologic diagnosis was clear cell carcinoma. Result of pleural fluid analysis for differential diagnosis between tuberculosis pleurisy and malignant pleural effusion was positive for carcinoma. The surgical stage of the patient was International Federation of Gynecology and Obstetrics stage IVA.
Between December 2015 and March 2016, the patient received 6 cycles of adjuvant chemotherapy consisting of paclitaxel (Taxol®; Bristol-Myers Squibb Company, Princeton, NJ, USA) and carboplatin (Paraplatin®; Bristol-Myers Squibb Company) every 3 week. On April 2016, just one month after the last chemotherapy, her level of CA-125 was increased to 52.4 U/mL compared to 20.5 U/mL on March 2016. On April 2016, abdominopelvic CT indicated hepatic metastasis and peritoneal nodularity in right paracolic gutter with interval increase in amount of ascites. These were interpreted as progression of the disease.
Chemotherapy regimen was changed to biweekly bevacizumab (Avastin®; Genentech, Inc., South San Francisco, CA, USA) and weekly topotecan (Hycamtin®; GlaxoSmithKline, Research Triangle Park, NC, USA) on April 2016. When the 5th cycle was done on September 2016, she presented slight pruritus erythematous patches on anterior chest wall and both breast skin. Dermatologist suggested topical steroid on impression of allergic contact dermatitis. She then finished 6 cycles of changed regimen until September 2016.
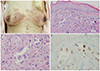
On October 2016, 21 days after 6th biweekly bevacizumab and weekly topotecan chemotherapy, the patient visited emergency department because of vomiting, diarrhea, and abdominal pain. abdominopelvic CT demonstrated possible perforation at the pelvic ileal loop. We performed small bowel resection and anastomosis, adhesiolysis, and peritoneal washing. During recovery, on October 2016, 11 months after the initial diagnosis, she complained that patch sizes on both breast skin were increasing (Fig. 1). We performed breast skin biopsy. Histological results including immunohistochemistry revealed metastatic adenocarcinoma (Fig. 1). She had consultation with the radiation oncology department. They did not recommend local external beam radiation therapy to the site of skin metastasis.
Fig. 1
(A) Multiple skin metastases on the anterior chest wall including bilateral breast skin: pruritus erythematous patches metastatic clear cell carcinoma in the dermis. (B) Tumor cells exhibit abundant eosinophilic cytoplasm and marked nuclear atypia in hematoxylin-eosin staining (×200), (C) hematoxylin-eosin staining (×400), (D) Immunohistochemistry for progesterone receptor is weakly positive within the metastatic clear cell carcinoma (×400).
On October 2016, due to complaint of cough and dyspnea, chest computed tomography evaluation was performed for the patient. It demonstrated newly appeared diffuse thromboembolism involving right main pulmonary trunk, right upper, middle, and lower lobar pulmonary arteries. We started anticoagulation treatment without chemotherapy because ileus was not controlled well by aggravating carcinomatosis peritonei. Approximately one month later, weekly paclitaxel chemotherapy was tried because the patient wanted to continue active treatment. Despite the patient had anticoagulation treatment and bilateral pleural percutaneous catheter drainage, her dyspnea, desaturation, and tachypnea were worsened progressively due to pulmonary embolism. Finally, on December 2016, the patient expired from cardiopulmonary arrest.
Discussion
In 2017, 22,440 cases of ovarian carcinoma and 14,080 deaths were reported in United States [1]. Among gynecologic malignancies, ovarian carcinoma has high mortality. In Korea, ovarian carcinoma is also the leading cause of death in gynecologic malignancy. It can be explained by the fact that most patients are presented at advanced stage with distant metastases. Dauplat et al. [2] have recognized that cytoreductive surgery and chemotherapy can be sued for local tumor control. However, many patients are dying with distant metastases. Frequently involved sites are the pleura, liver, lungs, and lymph nodes beyond pelvic and para-aortic chains.
Skin metastases rarely occur, with incidence ranging from 1.9% to 5.1%. The common sites of skin metastases are the abdominal wall, chest wall, and breast [2]. Kim et al. [8] have reported a rare lower extremities skin metastasis of papillary serous ovarian cancer. Matsui et al. [9] have presented a scalp metastasis of a serous ovarian cancer. Lee et al. [10] have noted one case of cutaneous metastatic carcinoma at right thigh from ovarian clear cell carcinoma (Table 1).
Table 1
Review of the literature of skin metastases in epithelial ovarian carcinoma

| Authors | Case No. | Interval (mon) | Metastatic site | Treatment | Overall survival (mon) |
|---|---|---|---|---|---|
| Dauplat et al. [2] | 9 | 31.9a,c) (range, 4 to 77) | Abdomen (7), chest wall (2), breast (1), right buttock (1)d) | Not applicable | 12.0b,c) (range, 1 to 41) |
| Cormio et al. [7] | 9 | 23.4a) (range, 4 to 37) | Chest and abdominal wall (6), surgical scars (3) | S+CT (4), CT (5) | 5d) (range, 2 to 65) |
| Kim et al. [8] | 1 | 42 | Lower extremities | S+CT | 5 |
| Matsui et al. [9] | 1 | 29 | Scalp | CT+RT | 12 |
| Lee et al. [10] | 1 | 71 | Lower extremities | CT | Not applicable |
| Schonmann et al. [11] | 1 | 36 | Lower abdomen, lower extremities, gluteal skin | CT | 1 |
| Charalampos et al. [15] | 2 | 24 (case 1), 120 (case 2) | Chest, abdomen, upper and low extremities (case 1), back (case 2) | CT (case 1), RT (case 2) | 14 (case 1), 24 (case 2) |
Several theories of mechanisms of skin metastasis in ovarian cancer have been proposed, including direct invasion from underlying growth and adjacent to extension of cells through lymphatics. Accidental cancer cells implantation during surgical procedures could also result in skin metastasis [345]. Some cases have shown the development of skin metastases in surgical scars (laparotomy scar, trocar port site, drainage scar, and port and catheter scar) [7].
There is usually a long-time between diagnosis of malignancy and skin metastases. Skin involvement signifies a widespread systemic disease. It is associated with poor prognosis [6]. Cormio et al. [7] have indicated that the median interval time between diagnosis of ovarian carcinoma and recognition of skin metastasis is 24 months. Dauplat et al. [2] have also suggested that the median interval time is 31.9 months (range, 4 to 77 months).
Clinical presentation of skin metastases can vary with a wide morphologic spectrum. Some skin lesions of metastases mimic other dermatological conditions such as herpes zoster eruptions, cellulitis, and erysipelas [611]. Our patient's skin lesion resembled contact dermatitis due to wire of underwear lining both breasts. Therefore, when skin has suspected lesion, a biopsy should be considered to confirm a diagnosis.
A few studies have presented local treatment of skin lesion such as surgical resection, electrocoagulation for extensive cutaneous metastases, electron beam therapy for large areas, and hematoporphyrin derivative injection with infrared phototherapy [7121314]. However, skin metastases appear in the late course of the disease, signifying disseminated and co-existing intraperitoneal disease. Patient with skin metastases would have already received several regimens of chemotherapy. This means that the patient is also resistant to cytotoxic drugs. Therefore, treatment depends on the patient's general condition, subjective symptoms, and objective signs of the lesion. To treat systemic disease, palliative chemotherapy could be considered first. Cormio et al. [7] have noted that patients with surgical excision followed by chemotherapy of skin metastatic lesions have longer median survival compared to patients with only chemotherapy. For limited skin metastatic lesion, surgery can be helpful. Fortunately in our case, she had no symptom of skin lesions such as itching sense, pain, signs of hemorrhage, or infection.
The median survival from diagnosis of skin metastases can vary from 4 to 24 months. Cormio et al. [7] have reported that the median survival from diagnosis of skin metastases is 4 months while Dauplat and Colleagues [2] have reported a median survival of 12 months. Charalampos et al. [15] have shown 2 cases with survival time after skin metastases of 1 year in the first case while the patient in the second case is still alive after 2 years. In the present case, the patient died 2 months later from the diagnosis of skin metastases.
In summary, we report the first case of skin metastases from ovarian clear cell adenocarcinoma in Korea. Clinicians should consider the possibility of skin metastases when patient complains skin lesions, especially in the abdomen and chest wall in a patient with ovarian carcinoma. Diagnosis is difficult based on clinical presentation with gross morphology of skin lesion. Skin biopsy needs to be performed. The optimal treatment for skin metastases from ovarian clear cell adenocarcinoma is currently unknown. The prognosis of most patients with skin metastases from ovarian clear cell adenocarcinoma is poor. Palliative treatment is needed depending on the patient's status.
 XML Download
XML Download