

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The interstitial part of the fallopian tube, the proximal portion that lies within the muscular wall of the uterus, is 0.7 mm wide and approximately 1 to 2 cm long [1]. Interstitial pregnancy is an uncommon kind of ectopic pregnancy and defined as a pregnancy in which the product of conception is implanted in the intramural portion of the fallopian tube [2]. Ectopic pregnancy accounts for approximately 2% of all recognized pregnancies, while interstitial pregnancy accounts for fewer than 3% of all ectopic pregnancies [3]. Although the overall ectopic pregnancy mortality rate has decreased dramatically from 72% to 90% in 1880 to 0.14% in 1990, the maternal mortality rate of interstitial pregnancies remains 2% to 2.5% [4]. Once the interstitial pregnancy ruptures, severe hemorrhage occurs because of the rich supply of blood vessels in the cornual region [5].
Known predisposing factors for interstitial pregnancies are previous ectopic pregnancy, previous salpingectomy, in vitro fertilization and embryo transfer (IVF-ET), ovulation induction, and sexually transmitted disease [6]. Recently, with the increasing incidence of in vitro fertilization attempts, the incidence of interstitial pregnancy is expected to increase. The traditional treatment of interstitial pregnancy was surgery including hysterectomy and cornual resection by laparotomic or laparoscopic approaches. This may adversely affect subsequent pregnancies with the possibility of uterine rupture during subsequent pregnancies. Several medical treatments, such as local potassium chloride (KCl) injection and methotrexate (MTX) treatment, have been introduced with generally satisfactory results [17].
MTX has been introduced and adopted as the first-line treatment for unruptured tubal pregnancy instead of salpingectomy. However, for interstitial pregnancy, there is limited number of data that demonstrates the treatment result of MTX and predicting factor for treatment outcome because of its rarity. There is no consensus of mode of treatment with MTX. In addition, there are limited data about pregnancy outcomes after MTX treatment. Therefore, this study aimed to evaluate whether MTX treatment for interstitial pregnancy is feasible and examine predictive factors for MTX treatment success. This study will provide information about pregnancy outcomes after MTX treatment in patients with interstitial pregnancy.
Materials and methods
This study was approved by the institutional review board of CHA Gangnam Medical Center (GCI-15-13). After obtaining institutional review board approval, the authors retrospectively reviewed the medical records of the patients who were diagnosed with interstitial pregnancy and underwent MTX treatment at CHA Gangnam Medical Center between January 2003 and July 2014. We collected patient demographics, treatment regimen, doses administered, treatment results, and subsequent pregnancy outcomes. In our institution, the diagnosis of interstitial pregnancy was made by transvaginal ultrasonography (TVU) using the following criteria: 1) no visible gestational sac within the uterus; 2) a gestational sac visualized in the fundus that is not surrounded by >5 mm of myometrium in all planes; and 3) a gestational sac seen separately and <1 cm from the most lateral edge of the uterine cavity.
Non-surgical treatment consisted of a systemic intramuscular MTX injection with or without a local MTX injection (1 mg/kg body weight) into an ectopic lesion under TVU guidance. For the systemic MTX injection, various regimens such as an 8-day alternating MTX regimen (1 mg/kg intramuscularly on days 1, 3, 5, and 7) [8], a single-dose MTX regimen (50 mg/m2 intramuscularly on day 1) [9], and a high-dose MTX regimen (100 mg/m2 + 200 mg/m2 intravenously over 12 hours) [10] have been used since 2003 (Table 1).
Table 1
Treatment regimens

For the local injection of MTX, patients emptied their bladders, prepared aseptically, and placed in the lithotomy position. Under propofol anesthesia, the ultrasonography probe was placed along the posterior wall of the vagina and directed at the interstitial ectopic mass. Using a 17-gauge 35-cm aspiration needle (Cook Australia, Queensland, Australia), a needle puncture into the gestational sac, followed by the injection of MTX (1 mg/kg body weight) into the gestational sac [11]. The presence of hemoperitoneum was checked before and after treatment. The procedure was well tolerated by patients and no major complications were recorded.
Treatment success was defined as the resolution of serum beta-human chorionic gonadotropin (β-hCG) levels without the need for surgical intervention. Treatment failure was identified if the patient required surgery.
The statistical analysis was performed using International Business Machines (IBM) Statistical Package for the Social Sciences statistics software version 22 (SPSS; IBM Corp., Armonk, NY, USA). The Mann-Whitney U test and χ2 test were performed to compare intergroup differences. The statistical analysis was also used to identify predictive factors of MTX treatment success of interstitial pregnancy. Values of P<0.05 were considered statistically significant. The statistical power was calculated using G*POWER 3.1.9.2 (Institut für Psychologie, Christian-Albrechts-Universität zu Kiel, Kiel, Germany).
Results
A total of 2,412 cases of ectopic pregnancy were diagnosed at the institution; of them, 97 (4%) were interstitial pregnancy. Among those patients, 38 hemodynamically stable women with unruptured interstitial pregnancy were initially treated with MTX. Patient demographics are presented in Table 2. The median patient age was 32.5 years (range, 24.0 to 40.0). The median serum β-hCG level was 4,327 mIU/mL (range, 375 to 102,970). Median size of the ectopic mass was 1.4 cm (range, 0.7 to 4.3). Median size of the gestational sac was 0.9 cm (range, 0.35 to 1.7). The yolk sac was observed in 11 patients. Fetal heart beat was observed in 3 patients. Median gestational week was 6+3 weeks (range, 5+0 to 11+3). The ectopic mass was within the left uterine cornus in 14 patients and right uterine cornus in 24 patients. Thirteen women (34.2%) had a history of previous ectopic pregnancy, while 23 patients (60.5%) had a history of at least 1 previous pelvic surgery. Thirteen women (34.2%) underwent either IVF-ET or intrauterine insemination.
Table 2
Patient demographics

Six patients were initially treated with a combination of systemic MTX and local MTX injected directly into the gestational sac under TVU guidance. Two patients were treated with local MTX injection only. Thirty patients were initially treated with systemic MTX only. Of those 38 patients who were treated with MTX, 21 were initially successfully treated with MTX treatment, while medical treatment failed in 17 and surgery was required. Seven patients had a β-hCG level >10,000 mIU/mL. Among them, 3 patients were treated successfully by MTX. One patient with a β-hCG level of 102,970 mIU/mL was successfully treated by systemic MTX. Another patient with a β-hCG level of 59,090 mIU/mL was treated by local MTX. Six women were at relatively advanced gestational age (>8 weeks); of them, 5 were successfully treated with MTX.
To investigate predictive factors for treatment outcomes, we compared variables between the MTX treatment success and failure groups including β-hCG, ectopic mass size, gestational sac size, crown rump length, presence of yolk sac, and gestational weeks at the time of diagnosis (Table 2). Only mode of MTX treatment was a significant predictive variable of treatment outcomes.
In the systemic MTX treatment group, 14 patients were successfully treated with intramuscular MTX injections and 16 patients underwent surgery. However, among patients who received treatment including local MTX injection, only 1 patient was failed to respond to MTX treatment. We evaluated whether the demographic differences between these 2 groups affected treatment outcome (Table 3). There were no demographic differences between the systemic MTX only and the local MTX (with or without systemic MTX) treatment groups except for the presence of yolk sac. We conducted a power analysis with α error=0.05 and effect size=0.5 and obtained a result of 0.533.
Table 3
Patient demographics in systemic vs. local MTX group

We examined the subsequent pregnancy results of the patients who were initially treated with MTX in our institution. Of the 38 patients who were treated with MTX, 17 patients were lost to follow-up. Among the other 21 patients, 13 patients (7 treated with MTX only and 6 who underwent surgery) attempted a subsequent pregnancy using assisted reproductive technology (ART). One woman with an elevated serum β-hCG after IVF-ET was diagnosed with an early pregnancy was transferred to another hospital for prenatal care. We excluded that case because the pregnancy outcome was lacking. Two women failed to achieve pregnancy. One woman had a tubal pregnancy on the same side of previous interstitial pregnancy that was treated by a systemic MTX injection. Consequently, 10 women had a pregnancy confirmed by ultrasonography for a subsequent pregnancy success rate of 83.3% (10 out of 12). Of those 10 women who delivered their baby after interstitial pregnancy treatment, 5 reached term and 5 delivered before 37 gestational weeks (Table 4). Nine of the 10 women delivered by cesarean section.
Table 4
Pregnancy outcomes
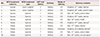
MTX, methotrexate; ART, assisted reproductive technology; C/S, cesarean section; PROM, premature rupture of membrane.
a)Four years later, this patient achieved subsequent pregnancy through ART followed by elective cesarean delivery of 1 healthy live baby at 37+5 weeks of gestational age; b)This patient just answered she had delivered single elective delivery in other hospital without commenting more information about the delivery.
There was one case of uterine rupture at 33+5 weeks. The patient was 30-year-old primigravidarum diagnosed with right interstitial pregnancy at amenorrhea 6+0 weeks. She was initially treated with MTX 75 mg intramuscular injection, but the serum β-hCG level increased from 4,050 to 16,100 mIU/mL and the ectopic mass enlarged from 1.3 to 1.7 cm. Therefore, she underwent laparoscopic cornual resection. After the surgery, she underwent IVF-ET, became pregnant with twins, and underwent cesarean delivery due to ipsilateral cornual rupture.
Discussion
Interstitial pregnancy is a rare but dangerous form of ectopic pregnancy whose incidence would be increased due to increased use of ART procedures. Although various approaches to treating this disorder have been previously reported, the optimal treatment regimen has not been determined due to its rarity [5].
In our study, the overall incidence of interstitial pregnancy was 4.0% (97 out of 2,315) of all ectopic pregnancies, which is comparable to those of previous reports [1]. The risk factors for interstitial pregnancy are previous pelvic surgery, previous history of ectopic pregnancy, and pregnancy after ART procedures.
This study revealed that MTX treatment mode was the only predictive factor of MTX treatment success. The overall success rate of systemic and/or local MTX therapy for treating interstitial pregnancy was 55.3%. Although there were no life-threatening events during treatment, the systemic MTX treatment group had a treatment success rate of 46.7% (14 of 30). Since Tanaka et al. [12] reported the first successful treatment of interstitial pregnancy with systemic MTX, several authors presented their experiences with MTX treatment for treating interstitial pregnancy. Lau and Tulandi [4] reviewed 40 additional publications in which the patients were treated with various regimens including systemic, local, and combined MTX treatment. The most commonly used regimen was an 8-day alternating MTX regimen (1 mg/kg intramuscularly on days 1, 3, 5, and 7). The authors showed that 83% (34 of 41) of patients were successfully treated conservatively. Hiersch et al. [13] reported a 70.5% success rate (12 of 17) for interstitial pregnancy using intramuscular MTX treatment consisting of an 8-day alternating (9 cases) or single-dose (3 cases) injection. In addition, Tanaka et al. [14] demonstrated a 93.9% success rate with intravenous MTX 300 mg with folic acid rescue for treating interstitial pregnancy. The success rates reported by other researchers were higher than ours. The high failure rate of our systemic MTX treatment was because of the regimen that we primarily used. Most of the patients who received systemic MTX therapy (24 of 30) were treated with a single dose regimen in our study. In addition, treatment failed in most of those who received a single dose of MTX (Table 1). These patients required 1 or 2 additional doses. Only 8 of 24 patients were successfully treated with the single-dose regimen. However, there was one failure of the 6 patients treated with a larger amount of MTX including the 8-day alternating and high-dose MTX regimens. Jermy et al. [15] reported a 94% success rate after single-dose intramuscular MTX injection in their prospective study of 17 interstitial pregnancy patients. Although the median β-hCG level was 6,452 IU, which is higher than ours (4,327 mIU/mL), 7 patients who were enrolled in the study had a β-hCG level <2,000 mIU/mL and 5 had a β-hCG level <1,000 mIU/mL. In our study, only 3 subjects had a β-hCG level <2,000 mIU/mL and only 2 had a level <1,000 mIU/mL. We assume that this was attributable to the differences in patient characteristics and the regimens that we adopted.
The systemic route of administration offers advantages over local injection into the ectopic gestational sac since it is less invasive and not operator-dependent, while local injection is a technically more challenging method, more invasive, and requires special devices and a skillful operator [1]. However, the systemic MTX treatment failure rate was 53.3% in our study. On the other hand, the success rate of the local MTX treatment group with or without a single-dose systemic MTX injection was 87.5% (7 of 8 patients), and local MTX treatment failed in 1 patient. Benifla et al. [11] reported a 66% (2 of 3 patients) success rate for ultrasound-guided local MTX injection with no severe side effects. Furthermore, Hafner et al. [16] and Timor-Tritsch et al. [17] reported a 100% of success rate for local MTX injection. Taking these results together, medical treatment such as combination of local MTX injection into the ectopic gestational sac and systemic single-dose MTX treatment might increase the MTX treatment success rate.
There are limited studies of the reproductive outcomes of interstitial pregnancy treatment. Benifla et al. [11] reported a 75% pregnancy success rate and made no mention of complications such as uterine rupture. Sagiv et al. [7] reported a 67% pregnancy success rate (6 of 9 patients); of them, 1 had an early miscarriage and 5 pregnancies reached term delivery. In this study, although all women were pregnant after ART procedures, those who were diagnosed with interstitial pregnancy and treated with MTX or surgery showed favorable pregnancy success rates. Successful subsequent pregnancy is likely after the successful treatment of interstitial pregnancy.
Uterine integrity after conservative treatment is unclear. Lau and Tulandi [4] proposed elective cesarean section as a wise delivery method after the conservative treatment of interstitial pregnancy following a case reported by Downey and Tuck [18]. They reported a case of a right interstitial pregnancy that resolved spontaneously after excision of a corpus luteum [4]. In our study, almost all patients (9 of 10) who were pregnant after the treatment of interstitial pregnancy underwent cesarean section for delivery. No patients who received MTX treatment only experienced uterine rupture. Despite the lack of a precedent, we considered vaginal delivery for patients in the conservative treatment group to maximize the advantages of avoiding surgery. Further studies are required to determine the feasibility of vaginal delivery after MTX treatment in patients with interstitial pregnancy.
However, among the patients who received surgical treatment, there was one case of uterine rupture at 33+5 weeks of pregnancy. Although the exact risk of uterine rupture in a subsequent pregnancy is unknown, women should be counseled carefully about the possibility. These patients largely achieved a subsequent pregnant with twins using IVF-ET. Therefore, patients treated surgically for interstitial pregnancy should consider a single rather than multiple embryo transfer to avoid having twins.
Our study has several limitations. There was a lack of consensus about systemic or local MTX treatment dosage because of its retrospective nature. In addition, because of the rarity of interstitial pregnancy, the study duration was >10 years. That is another reason various regimens were used in our institution. Second, the case number is too small to make a definitive conclusion. Third, the complications and side effects of MTX treatment could not be examined. However, there were no cases in which the MTX treatment was stopped due to drug toxicity and no complications occurred during the local MTX injection.
The main strength of our study is that entire sample size was relatively large. Second, we could compare the treatment success rates of local MTX injection and systemic MTX injection.
In conclusion, combined MTX treatment including local injection might be an appropriate initial approach for the treatment of unruptured interstitial pregnancy in hemodynamically stable women. MTX treatment also shows a favorable subsequent pregnancy outcome with an 83.3% pregnancy success rate. However, a prospective multicenter study is warranted to confirm the efficacy and safety of MTX combination treatment instead of surgical treatment as the first-line treatment for interstitial pregnancy.
 XML Download
XML Download