

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Placenta previa describes a placenta implanted in the lower uterine segment with complete or incomplete coverage of the internal cervical os [1]. It is well-known that massive postpartum hemorrhage (PPH) can develop in cases of placenta previa, increasing the risks of maternal and neonatal mortality and morbidity [23]. In such cases, prediction of postpartum blood loss improves the outcomes of pregnancy and yields information useful in the preparation for, and management of, surgery, including the need for hospital admission, reservation of blood supplies, and timing of cesarean section.
In most studies about placenta previa, postpartum bleeding was not massive because cases requiring only 1 pint of packed red blood cells (p-RBC) were defined as massive bleeding cases. However, what matters is not just mild or non-massive bleeding but massive postpartum bleeding needs prompt aggressive treatments. Meanwhile, although placenta previa is associated with PPH, massive PPH does not always develop. Most obstetricians consider that massive PPH occurs less frequently in patients with incomplete placenta previa, in whom the placenta is primarily located on the posterior uterine wall. Nevertheless, an incomplete placenta previa may also trigger massive PPH [4].
Therefore, the aim of the present study was to identify factors associated with massive PPH in pregnancies complicated by an incomplete placenta previa located on the posterior uterine wall.
Materials and methods
We performed a retrospective case-control study of data collected between January 2006 and April 2016. Of 718 pregnant women with placenta previa who delivered infants between 24 and 41 weeks of gestation, we excluded those with multiple pregnancies or diagnosed medical diseases during pregnancy. We also ruled out 296 cases with complete placenta previa or anterior placenta previa. Finally, we identified 210 singleton pregnant women with incomplete placenta previa located on the posterior uterine wall. The Institutional Review Boards (IRB) of CHA Bundang Medical Center approved this study (IRB No.2016-05-048-001). We reviewed the clinical records of the mothers and babies in terms of maternal demographics, clinical presentations, and ultrasound assessments.
Each placenta previa was diagnosed by an experienced obstetrician based on transvaginal ultrasound indications after 24 weeks of gestation. Diagnosis was confirmed within the week before delivery. An incomplete placenta previa was diagnosed when the placenta only partially covered the internal cervical orifice or was situated within 2 cm of the orifice.
Massive obstetric hemorrhage has been variably defined. One definition used is the acute need for 4 or more units of p-RBC [5]. In this study, blood loss ≥2,000 mL during surgery, postpartum transfusion of ≥4 pints of p-RBC, cesarean hysterectomy, or uterine arterial embolization triggered by postpartum bleeding were defined as massive hemorrhages. Elective cesarean section was planned between 37 and 39 weeks of gestation.
The clinical factors considered were maternal age at delivery, parity, body mass index, the number of prior uterine curettages, a history of previous uterine surgery, myoma uteri status, cervical length within the week before delivery, gestational age (GA) at the first episode of antepartum vaginal bleeding after 20 weeks of GA, the number of antepartum bleeding events after 20 weeks of GA, the need for emergency cesarean section, and fetal presentation.
We reviewed ultrasound findings in terms of placental location, multiple lacunae (≥4) (defined as an irregular area of low echogenicity larger than 1 cm × 1 cm in the placental parenchyma), lack of a translucent zone (the clear zone being defined as the line of low echogenicity between the myometrium and the placenta), and uteroplacental hypervascularity evident on color Doppler imaging (Fig. 1).
Fig. 1
Ultrasound findings of placenta previa. Placental lacunae (arrow) consisting of irregular area of low echogenicity in the placental parenchyma (A), absent of echolucent area (ellipse) between uterus and placenta (B) and hypervascularity of the cervix on color Doppler (C).
BL, bladder; IO, internal orifice of the cervix; PL, placenta; UT, uterus.

Statistical analysis was performed using SPSS version 23.0 (SPSS Institute, Chicago, IL, USA). We analyzed discrete data using the χ2 test or Fisher exact test and continuous variables using Student's t-test and Mann-Whitney U test, as appropriate. The association between the ultrasound and clinical characteristics and postpartum massive bleeding was analyzed by univariable and multivariable analysis. A P-value <0.05 was considered statistically significant.
Results
A total of 210 patients underwent elective or emergency cesarean section. No maternal or neonatal death occurred. The maternal characteristics and neonatal outcomes are shown in Table 1. Massive bleeding developed in 23/210 (11.0%) cases (Fig. 2). The non-massive and massive bleeding groups differed in terms of maternal age, the number of prior uterine curettages, and the presence of accreta. The estimated blood losses of the 2 groups were 655.4±215.1 mL and 1,469.6±474.3 mL, respectively.
Table 1
Clinical characteristics of the study population
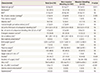
Fig. 2
Flow diagram for identification of participants with incomplete placenta previa located on the posterior uterine wall.

Table 2 shows associations between clinical and ultrasound factors and massive PPH. The non-massive and massive bleeding groups differed in terms are below.
Table 2
Association of clinical and ultrasound factors with the massive bleeding
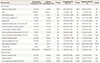
All characteristics were adjusted for maternal age, BMI, parity, prior uterine surgery, prior uterine curettage, myoma uteri, antepartum bleeding after 20 weeks of GA, uterine contraction at cesarean section, cervical length before delivery, GA at delivery, birthweight, placenta weight, gender, multiple lacunae, hypervascularity, and loss of hypoechoic retroplacental zone.
OR, odds ratio; CI, confidence interval; NS, not significant; BMI, body mass index; GA, gestational age.
Each marked data given as differently to *mean±standard deviation; †No. (%).
1) Maternal old age (≥35 years): 62 (33.2%) vs. 13 (56.5%), P=0.026
2) Two or more than 2 prior uterine curettages: 20 (10.7%) vs. 7 (30.4%), P=0.015
3) Placental multiple lacunae: 30 (16.0%) vs. 8 (34.8%), P=0.034
4) Uteroplacental hypervascularity: 59 (32.1%) vs. 17 (77.3%), P<0.001
5) Loss of hypoechoic retroplacental zone: 29 (15.5%) vs. 8 (34.8%), P=0.029
Univariate analysis revealed that maternal old age (odds ratio [OR], 2.62; 95% confidence interval [CI], 1.09 to 6.31; P=0.032), ≥2 prior uterine curettages (OR, 1.66; 95% CI, 1.52 to 5.36; P=0.018), fetal non-cephalic presentation (OR, 2.44; 95% CI, 1.48 to 12.57; P=0.012), placental multiple lacunae (OR, 4.97; 95% CI, 2.92 to 8.46; P<0.001), uteroplacental hypervascularity (OR, 7.13; 95% CI, 3.79 to 13.40; P<0.001), and loss of the hypoechoic retroplacental zone (OR, 2.49; 95% CI, 1.46 to 4.24; P=0.001) were associated with massive bleeding. After multiple regression, 4 variables were found to be associated with massive bleeding: ≥2 prior uterine curettages (adjusted OR [aOR], 4.47; 95% CI, 1.29 to 15.48; P=0.018), a short cervical length prior to delivery (<2.0 cm) (aOR, 7.13; 95% CI, 1.01 to 50.25; P=0.049), fetal non-cephalic presentation (aOR, 12.48; 95% CI, 1.29 to 121.24; P=0.030), and uteroplacental hypervascularity (aOR, 6.23; 95% CI, 2.30 to 8.83; P=0.001).
Discussion
Postpartum bleeding is associated with a risk of maternal mortality (about 140,000 deaths occur annually worldwide) [6]. Placenta previa is a high-risk factor for massive PPH [7], and increases the need for blood transfusion and cesarean hysterectomy [8]. The most commonly accepted risk factors associated with PPH in cases with placenta previa are a complete placenta previa and anterior localization of the placenta. A complete placenta previa is known to be associated with massive bleeding [91011]. We assume that the greater the proportion of the cervix is covered by the placenta, the greater the risk of bleeding. Also, anterior localization of the placenta was associated with massive bleeding in other studies [310]. We suggest that placental vessels penetrate other blood vessels supplying the bladder wall adjacent to the lower anterior region of the uterus, triggering massive bleeding during separation of the placenta from the uterus when the placenta is located anteriorly.
Meanwhile, most obstetricians consider that the risk of massive PPH is reduced in women in whom incomplete placenta previa are located on the posterior wall of the uterus. Although massive PPH occurs less frequently in cases with incomplete placenta previa, such women may also experience massive bleeding [4]. In our current study, we recorded massive PPH in 23 of 210 (11.0%) pregnancies with incomplete placenta previa. This result is consistent with that of a previous study in which 11.5% of women with incomplete placenta previa experienced significant postpartum bleeding [4].
Even if there have been no studies about massive PPH in cases with incomplete placenta previa located on the posterior uterine wall, some earlier studies identified risk factors for postpartum bleeding in cases with complete or incomplete placenta previa located on the anterior or posterior uterine wall. Mimura et al. [12] reported that a short cervical length (<2.5 cm) correlated significantly with massive bleeding during cesarean section of placenta previa patients. Another study revealed that advanced maternal age, a history of prior cesarean section, cervical hypervascularity, and a sponge-like finding of the uterine cervix were associated with massive PPH in women with placenta previa [9]. Oya et al. [8] found that advanced maternal age, prior dilatation and curettage, and a complete placenta previa were risk factors for a need for blood transfusion in women with placenta previa.
In the present study, we sought to define risk factors for massive PPH in women with incomplete placenta previa located on the posterior wall of the uterus. As in previous studies, we found that, even in such women, a history of prior uterine curettage, a short cervical length before delivery (<2.0 cm), and cervical hypervascularity were risk factors for massive PPH. Although the pathophysiology of such findings remains unclear, abnormal placentation and an initially poor blood supply to the placenta from the cervix and the lower segment of the uterine wall may cause the extent of uteroplacental vascularity to rise later in pregnancy [13]. We also found that fetal non-cephalic presentation greatly increased the risk of massive PPH in women with incomplete placenta previa. It is more difficult to extract the infant during cesarean section in cases with fetal non-cephalic than cephalic presentations, increasing the time from uterine incision to closure, and thus intraoperative blood loss.
In this study, the presence of placental multiple lacunae and the loss of hypoechoic retroplacental zone which have been considered as risk factors of PPH did not correlate with massive PPH. The trophoblasts tend to invade the myometrium and cause placental adherence to the uterine wall due to an absence or deficiency of Nitabuch's layer or the spongiosus layer of the decidua in cases with placenta previa. On ultrasound, placental multiple lacunae and the loss of hypoechoic retroplacental zone are known to be associated with the placental adherence [31214]. However, the lower segment of the posterior uterine wall is not equal to the anterior wall. They are different in the anatomy and routes of blood flow. Therefore, massive hemorrhage may not happen when the adherent placenta is located posteriorly, even if, in cases with anterior placenta previa, placental vessels which penetrate the blood vessels supplying the bladder wall tend to cause massive bleeding during separation of the placenta from the uterus.
Our study had a certain limitation. Because the work was a retrospective cohort study, some patient records and ultrasonographic images were not of perfect quality. Nevertheless, this is the first study on cases of incomplete placenta previa located on the posterior uterine wall, associated with massive PPH.
In conclusion, 2 or more prior uterine curettages, a short cervical length prior to delivery (<2.0 cm), fetal non-cephalic presentation and uteroplacental hypervascularity were found to be associated with massive PPH in cases with incomplete placenta previa located on the posterior uterine wall. Our findings may allow prediction of such bleeding and will enable obstetricians and multidisciplinary teams to prepare the necessary medical facilities more efficiently, including the equipment needed for massive transfusions, and schedule admission to the intensive care ward.
 XML Download
XML Download