

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Ovarian hyperstimulation syndrome (OHSS) is a serious complication in infertile women undergoing stimulated in vitro fertilization (IVF) cycle. The syndrome is characterized by massive ovarian enlargement, ascites, pleural effusion, adult respiratory distress syndrome, oliguria, electrolyte imbalance, hypoalbuminemia, hemoconcentration, thrombocytosis, and thromboembolic events [1]. Sometimes OHSS can be life-threatening and usually require long-term hospitalization for symptom resolution.
Cancellation of embryo transfer and freezing of all embryos can prevent late type OHSS, which occurred by endogenous human chorionic gonadotropin (hCG) produced by implanting blastocyst [2]. However, the freezing-all-embryo policy cannot prevent early type OHSS, which occurred by exogenous hCG for ovulation triggering [3].
Several strategies for prevention of early type OHSS have been suggested; coasting or use of modified ovulation triggering method such as low-dose hCG, recombinant luteinizing hormone (LH), or gonadotropin releasing hormone (GnRH) agonist. At the time of ovum pick up, administration of aspirin, methylprednisolone, cabergoline, IV albumin, or IV calcium was also suggested. However, none of those cannot eliminate early type OHSS completely [14].
After ovum pick up, prolonged administration of GnRH agonist was suggested to prevent development of early type OHSS [5]. In a non-randomized controlled trial, Endo et al. [6] administered a GnRH agonist for 7 days after hCG triggering in women undergoing freezing of all embryos due to a high risk of OHSS. The incidence of severe OHSS was significantly lower in the group in which GnRH agonist was continued, compared with the group in which GnRH agonist was discontinued. Prolonged administration of GnRH agonist might suppress ovarian enlargement and associated hormonal factors. However, a 5-day course of GnRH antagonist from the day of ovum pick up did not reduce the incidence of early type severe OHSS [7].
In patients developing fulminant early type OHSS, there are no definitive therapeutic medications that effectively treat an established OHSS. Lainas et al. [8] first reported a successful treatment of severe early type OHSS with daily administration of 0.25 mg GnRH antagonist (ganirelix, Antagon™; Organon Inc., West Orange, NJ, USA) for 7 days in 3 women, combined with freezing of all embryos. Quick regression of the syndrome was achieved without hospitalization in all patients and no complications were reported. They showed that 1-week course of GnRH antagonist might lead to rapid pituitary dysfunction and ovarian regression.
In a subsequent study by same researchers, daily administration of 0.25 mg GnRH antagonist (ganirelix) for 4 days successfully treated severe early type OHSS in 3 women with polycystic ovary syndrome [9]. In a subsequent study, embryo transfer was attempted and 2 women became pregnant and delivered healthy baby [10].
In a recent prospective cohort study by same researchers, daily administration of 0.25 mg GnRH antagonist (ganirelix) for 4 days combined with freezing of all embryos successfully treated severe early type OHSS in 40 women. None of them required hospitalization and severe OHSS rapidly resolved in all women [11]. In a study by other researchers, a 2-day course of GnRH antagonist (cetrorelix, Cetrotide®; Merck-Serono, Darmstadt, Germany) was also sufficient for treatment of early type OHSS [12].
From the above reports, we have administered GnRH antagonist (cetrorelix) in women developed severe early type OHSS after freezing-all-embryo since 2014. Here we report our treatment outcomes.
Materials and methods
1. Subjects
A retrospective analysis was performed after approval by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. B-1702-384-109). We administered GnRH antagonist (cetrorelix) in 10 hospitalized women for the treatment of severe early type OHSS admitted during November 2014 and July 2016. In 3 patients, oocyte retrieval was performed in our hospital, and in 7 patients, oocyte retrieval was performed in other clinics. Severe early type OHSS were developed 3–6 days after ovulation triggering (median, 3 days). All oocytes or embryos were frozen in all patients.
In 7 patients, GnRH antagonist protocol was used during ovarian stimulation, and GnRH agonist protocol was used during ovarian stimulation in 3 patients. In 6 patients, ovulation was triggered by recombinant hCG; dual triggering was used in 3 patients, and GnRH agonist triggering was used in 1 patient. Detailed ovarian stimulation outcomes in 10 patients were presented in Table 1. Before admission, no women received preventive measures except freezing all oocytes and embryos.
At admission, all women met the following criteria for severe early type OHSS; 1) presence of abdominal distension and/or dyspnea, 2) maximum diameter of ovary >7 cm, and 3) presence of ascites (depth of pocket >2 cm).
2. Management
Based on previous studies, GnRH antagonist (cetrorelix 0.25 mg per day) administration was planned for 4 days starting at the time of hospitalization, but the duration could be modified according to clinician's decision referenced by improvement of the patients' symptoms and signs [1011]. We informed all women about the off-label use of GnRH antagonist, and GnRH antagonist was used only in patients who consented to the use. The duration of administration was determined according to the improvement of the patient's symptoms and signs.
Conservative treatments such as fluid supplementation, drainage of ascites, and use of anticoagulant (enoxaparin 20 or 40 mg per day, Clexane®; Sanofi-Aventis, Paris, France) were performed as usual. Percutaneous indwelling catheter was inserted if patients were thought to be in need of frequent ascites drainage.
Vital signs and body weight was recorded daily. Blood tests including white cell count and hematocrit and trans-vaginal or trans-abdominal ultrasonography were performed every 1–2 days according to the patient's symptoms and signs.
Data are expressed as median (95% confidence interval [CI]). When the median value for clinical and laboratory parameters before and after GnRH antagonist was compared, the paired Wilcoxon signed rank test was used. A P-value of <0.05 was considered as statistical significance.
Results
Ovarian stimulation outcomes are described in Table 1. Two patients received 0.5 mg of GnRH antagonist for 1 day. GnRH antagonist 0.25 mg/day was used for 2 days in 3 patients, for 3 days in 4 patients, and for 4 days in 1 patient.
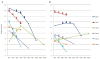
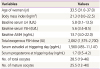
Several indices of body measurement, hematologic, laboratory, and ultrasonography before and after GnRH antagonist treatment and at the time of discharge are summarized in Table 2. Body weight, abdominal circumference, white blood cell (WBC) count, and hematocrits were decreased, and daily amount of urine output were increased during hospital course. The maximal diameters were significantly decreased in the right ovary but not in the left ovary.
In Fig. 1, maximal diameter of the right and the left ovary during hospital course are depicted in 6 patients. During hospitalization, trans-abdominal drainage of ascites by 18G needle was performed in 2 women (2 times for each). Drainage of ascites by percutaneous indwelling catheter was performed in 4 women. The median duration of indwelling catheter was 6 days (range, 2 to 11 days). Seven patients received daily anticoagulant.
In all patients, OHSS was successfully treated without any complication. The median duration of hospital stay was 6.6 days (range, 3 to 11 days). No side effect of GnRH antagonist was noted.
Discussion
In all patients, symptoms and clinical and laboratory indices were improved after GnRH antagonist administration. The median duration of hospital stay was 6 days (range, 3 to 11 days). Two out of 10 patients were hospitalized for more than 8 days. One patient received GnRH antagonist 3 times from the time of admission and overall symptoms were improved, however, cardiopulmonary symptoms such as bilateral leg edema, bilateral pleural effusion, and tachycardia persisted; this patient was discharged on the 10th day after cardiopulmonary work up. Another patient underwent IVF for oocyte freezing before chemotherapy for breast cancer; overall symptoms were improved after 2 doses of GnRH antagonist, but this patient was discharged on the 11th day because of management of neutropenia occurred after chemotherapy.
If hypovolemia and hemoconcentration are not corrected properly, prerenal insufficiency would be developed, which leads to oliguria and elevation of blood urea nitrogen (BUN) and creatinine [13]. When hypovolemia is corrected, the urine volume increases [14]. In our study, daily urine volume increased from 1,495 to 2,250 mL during GnRH antagonist treatment and it further increased to 3,510 mL at the time of discharge. Our result was similar to previous study, in which the daily urine volume increased from 1,889 to 2,660 mL after paracentesis of ascites [15].
In our series, both ovarian sizes were decreased during GnRH antagonist treatment. There was a statistically significant decrease in the diameter of the right ovary after treatment, but not in the diameter of the left ovary. Interestingly, initial median diameter was much greater in the right ovary than the left ovary (10.0 vs. 8.5 cm). This phenomenon might be associated with the findings that more oocytes were obtained in the right ovary after controlled ovarian stimulation [1617]. The frequency of ovulation in the right ovary was significantly higher than in the left ovary when comparing the frequency of ovulation in both fertile and infertile women (55% vs. 45%; P<0.05) [18]. The mechanism of an asynchrony in the activity of both ovaries is not yet clear but changes of inter-ovarian control mechanisms upon aging, and differences in innervation, vascular distributions, or anatomic asymmetry were suggested to explain the different response to ovarian hyperstimulation [16181920].
The role of the GnRH antagonist on the pituitary gland is primarily to decrease the secretion of endogenous LH. However, even in patients with OHSS, serum LH level in the luteal phase is low. Thus, direct ovarian action of GnRH antagonist has been suggested. GnRH receptors have been reported to be present in granulosa-lutein cells [2122]. Previous studies have shown that mRNA and protein expression for vascular endothelial growth factor (VEGF) and VEGF receptor are reduced in cultured human granulosa-lutein cell under GnRH antagonist administration [2324]. In a rat model, the GnRH antagonist administration reduced mRNA expression for VEGF and VEGF receptor in the hyperstimulated ovaries [24]. The use of GnRH antagonist in the luteal phase for rapid luteolysis has been reported in patients requiring rapid ovulation induction for cancer treatment [25]. In this case report, authors reported that rapid progesterone reduction after GnRH antagonist administration was observed and menstruation started 2–4 days later. In a previous study comparing functional changes and ultrastructural characteristics of natural luteolysis and GnRH antagonist induced luteolysis, luteolysis through GnRH antagonist treatment has been identified as involving proteins or cells different from naturally occurring luteolysis [26]. Thus, it is considered that the 2 processes occur with different mechanisms. Considering these results, GnRH antagonist administration may have different mechanisms than natural luteolysis and rapidly reduce the various vasoactive cytokines including VEGF produced by corpus luteum preventing the progression of OHSS.
Our study was a retrospective case series; therefore, there was no control group. In addition, small number of patients was included. Thus, prospective controlled studies with more patients will be needed in the future.
In conclusion, freezing of all embryos and GnRH antagonist administration appears to be safe and effective for women fulminant OHSS. Dose of GnRH antagonist and duration of its use should be further investigated.

 XML Download
XML Download