

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Dermoid cysts are one of the most common benign neoplasms, accounting for 10% to 20% of all ovarian tumors [1]. While ovarian dermoid cysts are usually asymptomatic, about 20% of patients with ovarian dermoid cysts can have complications, such as torsion (16%), rupture (1% to 4%), malignant transformation (1% to 2%), infection (1%), and invasion into adjacent viscera (<1%) [2]. Although ovarian dermoid rupture and fistula formation involving the bladder, rectum, and intestine are well documented in malignant transformation [34], fistula formation due to a benign ovarian dermoid cyst is a rare condition. To the best of our knowledge, laparoscopic repair of rectal fistula due to benign ovarian dermoid cyst has not been reported. Herein, we present a case of a benign ovarian dermoid cyst with a recto-ovarian fistula and successful laparoscopic repair of the rectal fistula.
CASE REPORT
A 17-year-old girl presented with lower abdominal pain, passage of sebaceous materials within the stool, and hematochezia for two months. She had no sexual relations and no specific medical or surgical history. The patient's vital signs on arrival were within normal limits, and she was afebrile. Physical examination revealed lower abdominal tenderness; however, there was no muscle guarding or rebound tenderness. Transrectal ultrasonography revealed a 10-cm heterogeneous cystic mass in the right ovary.
Laboratory studies revealed an elevated white blood cell count of 21.9 K/mm3 and a C-reactive protein level of 20.0 mg/dL. The results of tumor marker analyses performed preoperatively showed the following values: CA 125 95.3 U/mL (upper limit, 35 U/mL) and CA 19-9 69.9 U/mL (upper limits, 37 U/mL).
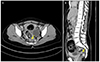
Computed tomography scan of the abdomen and pelvis revealed an 11×9×8-cm3 multilocular complex cystic mass thought to be a right dermoid cyst, which was seen to penetrate the middle part of the rectum (Fig. 1). A 5×5×4-cm3 complex cyst thought to be a dermoid cyst was also identified in the left ovary. The preoperative suspicion was an ovarian dermoid cyst that had ruptured and a recto-ovarian fistula. Therefore, the decision was made jointly by general surgeon and gynecologist to take the patient to the operating room for diagnostic laparoscopy and further procedures.
On laparoscopy, a large mass originating from the right ovary was seen, and it was contiguous with the rectum. There were extensive adhesions with the omentum and rectum, and preoperatively ruptured cystic contents were identified (Fig. 2A). A 5-cm mass was also identified in the left ovary. There was no torsion of both ovaries. After careful adhesiolysis, bilateral ovarian cystectomy was conducted and remnant ovarian tissues were closed using absorbable glyconate monofilament (MonoSyn 2-0, B. Braun, Tuttlingen, Germany). To identify the site of the rectal fistula, an air leak test was performed. We located the air bubble at the middle rectum. Perforation of the rectum was identified at the middle rectum (Fig. 2B). Primary repair was performed using 3-0 silk (Fig. 2C). After primary repair of the rectal fistula, we confirmed that there was no leakage during the air leak test. After the operation, massive irrigation was performed using Hartman solution (Fig. 2D). Histopathological examination revealed a benign dermoid cyst with acute suppurative inflammation.
The patient was treated with intravenous piperacillin/tazobactam for 10 days and her condition improved clinically. She was discharged in stable condition on postoperative day 12. The patient has been followed up regularly for the last 6 months.
Discussion
Rupture or perforation of the contents of a dermoid cyst into the adjacent viscera has been reported, with an incidence of less than 1% [1]. The urinary bladder is the most frequent organ involved in fistula formation. In the review of 38 cases of fistula formation of dermoid cysts, 30 fistulas involved the urinary bladder and the others communicated with the colon [5]. Fistula formation between a benign ovarian dermoid cyst and the large bowel and/or the rectum has been reported in a few cases [678].
The pathophysiology of fistula formation due to an ovarian dermoid cyst is not well understood. It is hypothesized that the mostly sebaceous cyst contents slowly leak into the abdominal cavity through a small rupture site, leading to a chemical granulomatous inflammation response. This causes adhesion between the cyst and the adjacent organs, such as the urinary bladder, small bowel, colon, or rectum. Circulatory disturbance and inflammatory response are probably responsible for the fistula formation [79].
Depending on the size of the dermoid cyst and the involved adjacent organ, clinical symptoms may include lower abdominal pain, rectal bleeding, or passage of dermoid cyst contents such as hair and sebaceous material, within the stool or urine. In this case, rectal bleeding and passage of sebaceous material within the stool were the main symptoms. Clinicians should be aware of the clinical findings of a rectal fistula due to ovarian dermoid cysts to avoid further life-threatening complications. Because malignant transformation is an important cause of the fistula [4], immediate access to accurate frozen section diagnosis and preparation of a surgical team for adequate cancer surgery is mandatory in suspected cases of fistula formation due to an ovarian dermoid cysts.
To the best of our knowledge, laparoscopic repair of a rectal fistula due to a benign ovarian dermoid cyst has not been reported. Only in one case report, laparoscopic surgery was attempted. However, there was conversion to laparotomy because of a full-thickness transverse colon defect [7]. Although fistula formation is suspected, the laparoscopic approach may be suitable for patients in terms of faster recovery times and better cosmetic outcomes. In addition, collaboration with experienced general surgeons is important to repair the fistula successfully.
In conclusion, a benign ovarian dermoid cyst complicated with rectal fistula formation is an extremely rare condition; however, awareness of the clinical and radiological findings in a recto-ovarian fistula is important to avoid further complications. In this case, a laparoscopic approach was successful and had the advantage of fast recovery time and a favorable cosmetic outcome; therefore, the laparoscopic approach may be considered for the treatment of a rectal fistula due to a benign ovarian dermoid cyst.

 XML Download
XML Download