

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Pregnancy complications including preterm birth (PTB), gestational hypertensive disorders, and fetal growth restriction (FGR) constitute substantial public health problems that are increasing in prevalence worldwide [1]. Many studies have sought to predict pregnancy complications. However, prenatal prediction of such complications remains difficult; no consensus has yet emerged on the most accurate and useful predictive parameters.
Several reports have indicated that fetal cardiac function yields important information on the hemodynamic status of, and cardiovascular adaptations in, women whose fetuses have perinatal complications [2]. Fetal echocardiograms are now commonly obtained at 20 to 24 weeks' gestational age (GA) to identify structural congenital heart disease. However, no study has yet investigated the utility of fetal cardiac function tests as predictors of pregnancy complications.
Therefore, we evaluated the ability of antenatal fetal cardiac output (CO), measured ultrasonographically at 20 to 24 weeks' GA to predict pregnancy complications (FGR, gestational hypertensive disorders, and PTB caused by preterm labor [PTL], or preterm premature rupture of membranes [PPROM]).
Materials and methods
1. Study population
We evaluated 133 fetuses at 20 to 24 weeks' GA. Women with medical conditions or multiple pregnancies, and pregnancies exhibiting fetal anomalies or abnormal estimated fetal weights (EFWs) (small for GA or large for GA) at the time of examination were excluded. In addition, 48 women who were transferred to local clinics for delivery were excluded from analysis. Ultimately, we enrolled 65 healthy mothers who gave birth at Ulsan University Hospital from November 2013 to August 2014. All women were informed about the aims of the study, and all gave written informed consent. The institutional review board of the Ulsan University Hospital approved this study (UUH 2015-01-001). Pregnancy complications included gestational hypertensive disorders (gestational hypertension, pre-eclampsia, and eclampsia), FGR, and PTB secondary to PTL and PPROM.
2. Echocardiography
A Voluson E8 ultrasound machine (GE Healthcare, Little Chalfont, Buckinghamshire, UK) was used in this study. Echocardiography was performed by an obstetrician specifically trained in the technique. CO was assessed by measuring the diameters (d values) of the left ventricle (LV) and right ventricle (RV) outflow tracts immediately above the aorta or pulmonary valve twice on frozen real-time images taken during systole using the leading-edge-to-edge method. Mean values were used in analysis. Aortic and pulmonary artery systolic time-velocity integrals and left and right heart rates were calculated from the same view by subjecting the areas beneath the Doppler spectra to planimetric evaluation (Fig. 1). Each left CO (LCO) and right CO (RCO) was derived using the following equation: CO (mL/min) = velocity time integral (cm) × π × d(cm)2/4 × heart rate (beats/min). Conventional atrioventricular flow velocity waveforms were obtained using apical four-chamber views. The Doppler sample volume was placed slightly distal to the mitral and tricuspid annuli, between the tips of the leaflets. Peak E and A wave velocities were recorded for atrioventricular flows, and the ratios of peak early vs. late transmitral flow velocity (E/A ratios) calculated. Fetal myocardial performance (Tei index) scores were also recorded. The end-diastolic dimension and end-systolic dimension of the LV and RV were measured in the ultrasonographic M-mode. The shortening fractions (SFs) of the LV and RV were calculated.
3. Other sonographic parameters
We also evaluated fetal growth and amniotic fluid volume. Fetal biometric measurements included the biparietal diameter, head circumference, abdominal circumference, and femoral length. Doppler measurements of the umbilical artery and middle cerebral artery (MCA) were also obtained. The umbilical artery systolic/diastolic ratio was measured in the umbilical cord in the region adjacent to the bladder. The peak systolic velocity of the MCA was measured distal to the junction of the internal carotid artery evident in the transverse view of the fetal skull. The measurement was made at the level of the circle of Willis.
4. Statistical analysis
Statistical analysis was performed using IBM SPSS ver. 19.0 (IBM Corp., Armonk, NY, USA). We analyzed discrete data using the Fisher's exact and continuous variables using Student's t-test or the Mann-Whitney U-test, as appropriate. We also performed a multivariate logistic regression analysis. A receiver-operating characteristic curve was constructed for the prediction of pregnancy complications by the LCO and RCO to the LCO ratio. Best cut-offs (points with the highest sensitivity and lowest rate of false positivity) were then established. A P-value <0.05 was considered statistically significant.
Results
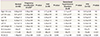
Sixty-five babies were delivered in our hospital. Table 1 lists the perinatal characteristics of mothers with and without pregnancy complications. In total, 23 had one or more pregnancy complications. There were nine cases of FGR (13.8%), eight of gestational hypertensive disorders (12.3%), and twelve of PTB caused by PTL or PPROM (18.5%). Several mothers experienced more than one complication.
We found no difference in maternal age, parity, mode of delivery, PTB history, or neonatal gender between mothers with and without pregnancy complications (Table 1). Furthermore, we found no between-group difference in GA or in MCA peak systolic velocity at the time of fetal cardiac function examination. However, significant between-group differences were apparent in maternal body mass index prior to pregnancy, EFW during measurement of fetal cardiac function, GA at the time of delivery, birth weight, and the incidence of a low Apgar score 5 minutes after delivery. The EFW was in the normal range because we excluded all cases with abnormal EFWs (e.g., small for GA or large for GA) from analysis.
There were no significant differences in the E/A ratio, Tei score, SF, or RCO (Table 2). However, LCO was lower in the patients with than without pregnancy complications (88±53 vs. 117±48 mL/min, P=0.028). The RCO/LCO ratio was higher (2.43±1.69 vs. 1.48±0.81, P=0.001). The RCO/LCO was higher in the FGR (2.21±1.38 vs. 1.48±0.81, P=0.046), gestational hypertensive disorders (2.11±1.49 vs. 1.48±0.81, P=0.043), and PTB subgroups (2.58±2.08 vs. 1.48±0.81, P=0.004) than in the normal group (Table 2).
Multivariate analysis of adjusted maternal age, body mass index, parity, PTB history, GA at measuring CO, and EFW demonstrated that the RCO/LCO ratio was a significant predictor of pregnancy complications (adjusted odds ratio, 7.76; 95% confidence interval [CI], 1.15 to 52.21; P=0.029) (Table 3). In each case, the RCO/LCO ratio was a significant predictor of gestational hypertension (adjusted odds ratio, 6.59; 95% CI, 1.17 to 37.14; P=0.032) and PTB (adjusted odds ratio, 2.36; 95% CI, 1.08 to 5.14; P=0.031) (Table 4).
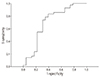
The area under the receiver-operating characteristic curve used to predict pregnancy complications from LCO was 0.71 (P=0.011) (Fig. 2). The diagnostic cut-off value used for LCO was 80 mL/min. The area under the receiver-operating characteristic curve derived from the RCO/LCO ratio was 0.68 (P=0.02) (Fig. 3), and the diagnostic cut-off value was 1.41 (68.2% sensitivity, 50.0% specificity).
Discussion
In this study, we demonstrated that ultrasonographic fetal CO measurement at a GA of 20 to 24 weeks is useful for the prediction of pregnancy complications. The complication rate was 35.4% (23/65), which appears high because 48 patients were transferred to local clinics after normal results of fetal heart function evaluation were obtained at our hospital.
Several studies that analyzed fetal cardiac function have indicated that such analysis provides important information on the hemodynamic status and cardiovascular adaptations during perinatal complications. Deterioration in clinical measures of cardiac function may frequently represent the first sign of fetal pathology [3].
Over the years, a number of different ultrasound methods have been proposed in an attempt to quantitatively evaluate fetal cardiac function, such as the E/A ratio, myocardial performance index (MPI), SF, and CO [34].
In a healthy fetus, the E/A ratio is typically <1 because the majority of the blood passing to the ventricle is propelled by atrial contraction due to reduced compliance of the ventricular myocardium [345]. In patients with a reduced E/A ratio, the process of ventricular filling depends more on atrial contraction than on negative pressure during relaxation. This occurs mainly during two conditions: chronic hypoxia and cardiac overload [56]. However, there are limitations associated with its use. For example, both the E and A waves are fused in cases of fetal tachycardia. In our study, there was no difference in the E/A ratio between patients with and without pregnancy complications.
The MPI has been shown to be relatively stable, varying only slightly throughout gestation (mean MPI, 0.36; range, 0.28 to 0.44) [7]. In our study, the mean MPI was 0.36±0.12. The MPI increases in hypervolemia and high cardiac afterload [8]. Benavides-Serralde et al. [9] reported that in cases of FGR, the MPI was a reliable early marker of fetal cardiac dysfunction. In the present study, however, there was no difference in the MPI between patients with and without pregnancy complications. MPI measurements have several limitations. Most importantly, this measurement method is non-reproducible and it is not easy to obtain a clear-cut waveform. Furthermore, because the MPI is easily affected by the heart rate, it is markedly more difficult to apply MPI measurement to fetuses, which typically have variable heart rates. Finally, there is variation in reference ranges previously reported among different research groups; universal agreement on machine settings and the valve click measurement phase is required [1011].
The SF represents the systolic decrease in ventricular diameter expressed as a ratio of the end-diastolic diameter using M-mode. The SF can reflect CO. However, standardization of the measurement is difficult due to problems with M-mode alignment [4]. In our study, SF did not differ significantly between patients with and without pregnancy complications.
Several reports have described the assessment of fetal conditions using CO, which is determined by stroke volume and heart rate. Under normal conditions, there is a continuous increase in all cardiac volumes throughout gestation, predominantly the RV volume, which accounts for 55% to 60% of the continuous CO [8]. Under hypoxic conditions, CO might respond differently due to a brain-sparing effect or cardiac overload. Much amount of blood ejected by the LV is forwarded to brain. And increased placental resistance is predominantly expressed in the RV because the blood flow which it ejects is mainly forwarded to the lower part of the fetal body and placenta. Therefore, the RCO/LCO ratio might be decreased [5]. However, there are several reports in which the increased afterload induced by placental insufficiency may have reduced the LCO because changes in tissue resistance in this region are reflected principally in the LV. Rizzo et al. [12] reported that the ejection force of the LV was significantly lower than that of the RV, while Kiserud et al. [13] found that the ejection force of both the LV and RV were decreased during FGR.
According to our data, CO (especially LCO) may be in a pathological state before clinical signs appear. This suggests that an obstetrician should monitor the occurrence of pregnancy complications if the fetal LCO is <80 mL/min or the RCO/LCO ratio is 1.41 on fetal echocardiograms performed at a GA of 20 to 24 weeks. Why the RCO was greater than the LCO in our study remains unclear. The RV may work harder than the LV to overcome placental resistance during early-stage pathology. As the disease progresses, the role of LV, which passes blood to the fetal brain, might increase. Finally, the RCO and LCO may be in balance, or the LCO could increase more than the RCO.
The novel findings of this study are as follows. First, this is the first prospective study to reveal that ultrasonographic fetal CO measurement at a GA of 20 to 24 weeks is effective for the prediction of pregnancy complications. Our study also provides evidence that in complicated fetal cases with normal umbilical artery and MCA Doppler values, the E/A ratio and MPI may represent signs of subclinical cardiac dysfunction. Second, this study proves that fetuses are already affected by pathologic conditions in the mid-trimester, although clinical signs later during later pregnancy. From a pathophysiological viewpoint, this fact is consistent with previous evidence that a proportion of fetuses exhibiting FGR and those under conditions of maternal preeclampsia are exposed to placental insufficiency and chronic restriction of nutrients and oxygen due to abnormal placentation during early pregnancy [11]. Third, our study provides important information on the changes in placental vascular resistance associated with PTB, resulting from PTL or PPROM. These findings may serve as a basis for future studies pertaining to pathologic conditions during PTB. For example, our data support other studies relating PTB to chronic placental inflammation [14].
However, there are also several limitations to our study. First, although we attempted to overcome the lack of reproducibility by employing a single trained obstetrician to perform all fetal echocardiographs, obtaining a standard method and objective reference values for fetal CO should be a target for future research. Second, measuring fetal CO requires extensive training and laborious data post-processing. Nevertheless, we believe that measurement of fetal CO has applicability for the assessment of specific pathologies or for use in research settings.
In conclusion, this study demonstrated for the first time that pregnancy complications such as FGR, preeclampsia, and PTB resulting from PTL or PPROM can be predicted based on fetal CO assessments made by ultrasonography at a GA of 20 to 24 weeks. In our opinion, measurement of fetal CO represents an additional informative parameter for the management of high-risk pregnancies because it effectively predicts prenatal complications during relatively early-stage pregnancy.





 XML Download
XML Download