

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
An umbilical hernia is a protrusion of the peritoneum, omentum, or a part of another abdominal organ through the umbilical ring, which commonly affects neonates and young children [1]. It accounts for 5% to 7% of all primary hernias in adults [12], and can be caused by an increase in intra-abdominal pressure due to pregnancy, obesity, ascites, and intra-abdominal tumors, or by weakness of the umbilical ring [3]. The herniation can cause rupture, strangulation, and, in rare cases, incarceration. Incarceration requires surgical repair of the hernia, and accounts for 10% to 20% of all operative cases [2].
Uterine fibroids are common benign tumors with a prevalence of approximately 25% in women aged older than 35 years [4]. Unless the fibroids cause symptoms or grow rapidly within a few months, they be may be managed conservatively [5]. However, several reports have described incarceration of a fibroid in an umbilical hernia, particularly during pregnancy [4567]. Here, we report a rare case of a fibroid presenting as an incarcerated umbilical hernia in a menopausal woman. To the best of our knowledge, this is the first case of a pedunculated fibroid in an umbilical hernia in a nonpregnant woman with large intra-abdominal fibroids.
Case report
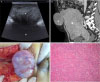
A 66-year-old woman presented with a palpable, pain-free mass in the umbilical region that had been present for 6 months. She had no symptoms suggestive of intestinal obstruction, such as nausea, vomiting, or abdominal distension. She had not undergone any abdominal surgical treatment, which ruled out the possibility of umbilical herniation as a postoperative complication. Although the patient had been taking an antihypertensive drug for 10 years and her body mass index was 28 kg/cm2, her general condition was good. Physical examination revealed a goose egg-sized firm, movable, and nontender mass in an umbilical lesion, without any surrounding inflammation. The initial laboratory results showed normal values, and the CA 125 level was 43.6 U/mL. Abdominal ultrasound showed an 8.5 cm×5.5 cm oval, hypoechogenic mass within the umbilical sac, connected to an intra-abdominal mass with a 3.6-cm umbilical fascial defect (Fig. 1A). Although the clinical impression was that of an incarcerated fibroid, multidetector computed tomography (MDCT) was also performed to rule out an abdominal wall desmoid tumor or direct abdominal wall metastasis of a gynecologic malignancy, such as ovarian cancer or leiomyosarcoma. MDCT revealed a huge intra-abdominal mass (20 cm×17 cm×14 cm) with diffuse inhomogeneous enhancement, a relatively well-demarcated border, and an 8-cm pedunculated subserosal fibroid in an umbilical hernia (Fig. 1B). Intraoperative findings showed an umbilical hernia sac containing an approximately 8 cm × 8 cm pedunculated fibroid, with the short stalk measuring 3 cm×3 cm, which was the umbilical defect (Fig. 1C). Abdominal hysterectomy was performed along with intraoperative assessment of frozen sections, which showed findings consistent with a benign uterine fibroid. The umbilical defect was repaired with primary suture. No complication was observed in the postoperative period, and histological examination confirmed that the uterine fibroid weighing 2.75 kg was of the cellular type (Fig. 1D).
Discussion
Incarceration of uterine fibroids in an umbilical hernia is a rare complication that has mostly been reported in pregnant women (Table 1) [1267]. In 1999, the first case of pedunculated fibroid incarceration in an umbilical hernia in a pregnant woman was reported [6]. A fibroid uterus is typically too small to reach the level of the umbilicus, and the intra-abdominal pressure is too low to cause herniation. Consequently, all reported cases of incarceration of an umbilical hernia occurred during pregnancy, especially in the third trimester, after 28 weeks of gestation [1267]. In the current case, the uterus was enlarged (2.75 kg) and exceeded the level of the umbilicus because of a huge fibroid, which was sufficient to cause herniation. And in postmenopausal women, with aging process, the weakness of abdominal wall would be another cause of herniation.
All previously reported cases were symptomatic and required emergency surgery for pain. However, in the current case, the pedunculated fibroid was entrapped in the umbilical hernia, as observed on MDCT. It remained asymptomatic because it was not stretched, in contrast to similar cases reported in pregnancy. Rapid uterine enlargement during pregnancy may displace the incarcerated fibroid cranially onto the anterior wall of the uterus, causing severe pain.
MDCT was performed because abdominal ultrasound failed to provide sufficient details of the anatomy of the herniated mass; this also ruled out ovarian malignancy or desmoid tumor of the abdominal wall. Although a uterine leiomyosarcoma could not be completely excluded before surgery, MDCT imaging helped make the preoperative decision to manage the mass as a herniated fibroid [8].
The reported size of herniated fibroids has varied from 3 to 10 cm. In fact, there is no consensus on the best technique for the repair of umbilical hernia in adults [9]. Arroyo et al. preferred mesh repair to primary suture for umbilical hernia with small defects (<3 cm) because of its low recurrence rate [10]. However, Kurzer et al. [11] did not observe any differences in recurrence rate between patients with small umbilical defects who underwent mesh repair and those who underwent primary suture, during a follow-up period of 43 months. In the current case, the herniated fibroid was >8 cm, whereas the umbilical defect was relatively small (3 cm×3 cm). Therefore, primary suturing of the defect was performed instead of mesh repair.
Hernia reduction and repair can be performed, under local anesthesia, with low morbidity and high patient satisfaction. Three of the four previously reported cases in pregnancy were also managed with the reduction method. However, we opted for abdominal hysterectomy under general anesthesia to confirm the absence of malignancy.
In conclusion, increased intra-abdominal pressure due to a huge fibroid may contribute to the herniation of the fibroid through the umbilicus. Therefore, the possibility of an incarcerated fibroid should be considered before checking for an abdominal wall tumor or a gynecologic malignancy when a patient presents with a solid, palpable umbilical mass combined with a huge pelvic mass.

 XML Download
XML Download