

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Borderline ovarian tumors (BOTs) are characterized by the presence of cellular proliferation and nuclear atypia without stromal invasion. They represent 10% to 15% of all epithelial ovarian tumors [1]. Compared to invasive epithelial ovarian cancers, BOTs typically present in younger women, are diagnosed at earlier stages, and have better prognoses [2]. The median age at diagnosis is 45 years, and 34% of patients are of childbearing age (under 40 years) [3]. The age at first pregnancy now exceeds 30 years in many developed countries [4]. Therefore, surgery for younger women diagnosed with BOTs has moved from radical treatment to a more conservative approach [5]. Fertility-sparing surgery (FSS) is safe, feasible, and widely accepted and performed [678]. Although many studies have investigated FSS in BOTs [9], data regarding specific obstetric outcomes among the different FSS subtypes are limited. The aim of the present study was to investigate the obstetric and oncologic outcomes of two FSS subtypes in reproductive-age women with BOTs.
Materials and methods
We reviewed the medical records of patients pathologically diagnosed with BOTs between 1998 and 2014. The study subjects included patients who underwent primary surgery at our institution as well as those referred for comprehensive staging operations after initial surgery at another clinic. Pathologically diagnosed with intraepithelial carcinoma or microinvasion was not included in this study. Subjects also had to be reproductive-age women (under 40 years) who were initially treated with FSS. FSS was defined as preservation of the uterus and at least part of one ovary. It was classified into two subtypes: unilateral salpingo-oophorectomy with or without contralateral ovarian cyst enucleation (USO), and unilateral or bilateral cyst enucleation (CE). Patients were treated with adjuvant platinum-based chemotherapy at the discretion of their physicians (Table 1).
Demographic, clinical, pathological, surgical, obstetrical, and follow-up data were extracted from the medical records. The pathology slides were reviewed centrally by two expert pathologists. Telephone interviews were conducted to assess obstetric outcomes such as menstruation, pregnancy attempts, successful pregnancy, and usage of assisted reproductive technology (ART). Disease recurrence rates and pregnancy rates were compared between the USO and CE groups. Recurrence-free survival was defined as the time from the initial surgery to disease recurrence or censor date. Survival curves and rates were calculated using the Kaplan-Meier method. The differences in survival were assessed using the log-rank test. Frequency distributions were compared using the chi-squared test and Fisher's exact test, and both mean and median values were compared between the two groups using the Student's t-test. A P-value of ≤0.05 in a two-sided test was statistically significant. All statistical analyses were performed using the SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). This study was approved by the institutional review boards.
Results
1. Patient characteristics
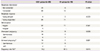
Of the 108 patients who met our inclusion criteria, 89 had undergone USO and 19 had undergone CE. The baseline patient characteristics are presented in Table 1. There were no significant differences in terms of age at diagnosis, CA 125 levels, surgical approach, parity, histological type, stage, peritoneal implant, and adjuvant therapy between the two groups. With regard to the histologic type, 28 were serous (25.9%), 72 mucinous (66.7%), and nine others (endometrioid, mixed cell type; 7.4%). After the initial surgery, nine USO patients USO (14.6%) and two CE patients (10.5%), who mainly had stage Ic and II BOTs, received adjuvant platinum-based chemotherapy. Nine patients received carboplatin with paclitaxel, and two received cisplatin with cyclophosphamide.
2. Oncologic outcomes
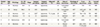
The median follow-up period was 37.4 months in the USO group, and 25.4 months in the CE group. Six patients developed recurrent disease 9 to 67 months after the initial surgery. The median recurrence-free interval was 24 months. The rate of recurrence was significantly higher in the CE group than in the USO group (15.8% vs. 3.4%, P=0.032) (Table 1). The 5-year recurrence free survival rate was significantly higher in the USO group than in the CE group (95.7% vs. 78.8%, P=0.022) (Fig. 1).
Table 2 summarizes the oncologic outcomes of patients with recurrent disease. All six patients had recurrent BOTs, none of which were invasive in nature. Regarding histologic subtypes, four were mucinous, one was serous, and one was seromucinous. Case 1 originally involved a 16-cm left ovarian cyst that was treated with left USO. After 41 months, a computed tomography scan revealed a right ovarian cyst that was treated with a right adnexectomy. The two other cases in the USO group involved recurrent disease in the contralateral ovary and uterus respectively, and were managed with radical surgery including hysterectomy. In the CE group, the sites of recurrence were the ipsilateral ovary, contralateral ovary and both ovaries. All three patients underwent a second FSS; in case 6 as well, six cycles of platinum-based adjuvant chemotherapy was administered at the time of surgery. There were no disease-related deaths, and all patients were alive with no evidence of disease after surgery.
3. Obstetric outcomes
Eighty-two (75.9%) of the 108 patients were contacted by telephone. Of these, six refused to participate in the interview, but the remaining 76 were able to provide information on their menstrual cycles and obstetric histories (Table 3). Of the 76 patients, 71 resumed regular menstruation and 5 had irregular menstruation; none experienced premature menopause. Four patients were pregnant at the time of FSS and had simultaneous cesarean sections. All four delivered healthy full-term babies.
Of the 73 patients with stage I BOTs, 31 attempted to conceive, of which 25 were successful. Of the three patients with advanced BOTs, one attempted to conceive and had two successful singleton pregnancies. In case 1 (Table 2), the patient developed a recurrent borderline tumor on the contralateral ovary, and succeeded in conceiving and delivering a full-term baby vaginally 32 months following her second FSS (USO).
In the USO group, 19 of the 24 women (79.2%) who attempted to conceive had a total of 25 pregnancies; this included two who underwent ovulation induction using clomiphene citrate and in vitro fertilization. These pregnancies resulted in 21 full-term deliveries. There were three spontaneous abortions and one ongoing pregnancy at the time of analysis. In the CE group, seven of the eight women (87.5%) who attempted to conceive had a total of eight pregnancies; this included one who underwent ovulation induction using clomiphene citrate and in vitro fertilization. These pregnancies resulted in seven full-term deliveries and one ongoing pregnancy. None of the patients underwent radical surgery after delivery.
Discussion
Fertility-sparing treatments are defined as procedures that preserve the uterus and some functional ovarian tissue [1011]. Several studies have compared the oncologic outcomes of radical surgeries and FSS [11121314]. However, few studies have compared the oncologic and obstetric outcomes of FSS subtypes (USO vs. CE) [1516]. One such study, which compared the oncologic outcomes of USO and CE, found that CE patients have a higher recurrence rate than USO patients [16]. These findings are consistent with the results of the present study, which found that the recurrence rate was significantly higher following CE (15.8%) as compared to after USO (3.4%, P=0.032) (Table 1).
In the present study, all six patients with recurrent disease had recurrent BOTs and not an invasive cancer. They were successfully treated with further surgery (Table 2). This was consistent with Song et al. [16]'s hypothesis, that despite the substantial risk of relapse following CE for BOT, this approach does not impair patient survival.
The histology of the BOT is also an important consideration. Mucinous type BOTs predominate in East Asia, including Korea [17]. A previous study on BOT types found that 31% were serous and 68% mucinous [17]; these numbers are similar to those of the present study's (26% vs. 67%) (Table 1). Recent studies suggest that mucinous-type BOTs may not be benign, and instead, have a 13 cumulative risk of recurrence in the form of invasive carcinoma at 10 years [1171819]. Uzan et al. [8] has also suggested that mucinous BOTs are ‘high-risk’ in that invasive recurrence is likely after FSS in stage I disease. Therefore, the authors of these studies concluded that USO is preferable to CE for patients with mucinous BOTs. In regions with a high prevalence of mucinous BOTs such as Korea, USO might be considered the FSS of choice rather than CE, consistent with the result of present study.
Regarding obstetric outcomes, the reported pregnancy rate for BOT patients ranges from 40% to 100% [2122021222324], although the use of different surgical approaches in those studies was limited. Vasconcelos and de Sousa Mendes [24] conducted a meta-analysis of 32 studies, and found that the pregnancy rate for women who underwent USO was 45.4% (n=21/46), and the rate for women who underwent CE was 40.3% (n=26/61). In the present study, 26 of the 32 patients (81.3%) who tried to conceive had successful pregnancies (Table 3). The pregnancy rates of the present study were 79.2% (n=19/24) in the USO group and 87.5% (n=7/8) in the CE group. Cystectomies tend to preserve fertility better than adnexectomies because less ovarian tissue is removed. However, in the present study, the pregnancy rates between the two groups were not significantly different (P=0.615). These results are consistent with those of a previous study [16], and suggest that the obstetric outcomes after USO or CE are promising. The majority of patients also had successful term pregnancies with no congenital anomalies.
Some researchers believe that the appearance of invasive implants on the peritoneal surface portends a less favorable prognosis in patients with BOTs [25]. As such, adjuvant chemotherapy can be considered for these patients, using the regimen typically used for epithelial ovarian cancer. However, studies have shown that postoperative adjuvant chemotherapy fails to lower the relapse rate or improve the survival rate in both the early and advanced stages of BOTs [2627]. This present study included 11 of 108 patients (10.2%) who received adjuvant chemotherapy. The majority had FIGO (International Federation of Gynecology and Obstetrics) stage Ic disease or above, and received the treatment before 2005 according to the discretion of their physician. Of the 11 patients who received adjuvant chemotherapy, only one (case 3 in Table 2) developed recurrent disease 67 months later. She then underwent successful radical surgery, whereupon no evidence of disease remained. An adverse effect was observed in one patient who developed grade 2 leukopenia. Four patients succeeded in conceiving spontaneously after chemotherapy, and delivered full-term babies. Considering the incidence of recurrence in this present study, there was no benefit to receiving adjuvant chemotherapy. This was consistent with the findings from previous studies [1282930]. As such, we would carefully conclude that adjuvant chemotherapy can be avoided for BOT patients with a strong desire to bear children.
This study had several limitations. First, it was a retrospective analysis that was limited to a single center. Second, comprehensive surgical staging was not considered for all subjects. Third, the length of follow-up was insufficient. Especially, in CE group, the median follow-up period was shorter as 25.4 months than USO group. Fourth, the obstetric outcomes were subjective and depended on telephone interviews. More objective parameters, such as preoperative and postoperative ovarian function (follicle stimulating hormone, anti-Mullerian hormone, antral follicle count), should have been included.
The strengths of the current study include the relatively large sample size. In addition to confirming the effectiveness of FSS as a treatment for BOT, the current study has demonstrated the favorable obstetric outcomes of FSS in women under 40, and has compared the pregnancy rates between two FSS subgroups (USO and CE).
In this study, the recurrence rates in patients with BOTs treated with USO (3.4%) were significantly lower than in patients treated with CE (15.8%) (P=0.032). In addition, both USO (79.2%) and CE (87.5%) had excellent obstetric outcomes. Therefore, USO is an appropriate fertility-sparing treatment for young women with BOTs. Meanwhile, in some patients, CE may be the only viable option due to their previous history of unilateral oophorectomy or salpingo-oophorectomy, or bilateral BOTs. In our study, all recurrent lesions were BOTs located in the remaining ovary, and were successfully treated by secondary surgery. Therefore, CE is still an acceptable option, but should be limited to selected patients.


 XML Download
XML Download