

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Hypertensive disorders of pregnancy are important and serious problems that affect both maternal and fetal morbidity and mortality. Preeclampsia is known to be typically characterized by new-onset hypertension, proteinuria, and other systemic disturbances; it is currently updated as a pregnancy-specific syndrome that affects virtually every organ system [1]. The diagnostic criteria for preeclampsia have changed with an increased understanding of its pathophysiology and the available evidence. According to a recent task force of American College of Obstetricians and Gynecologists (2013), preeclampsia can be diagnosed by the presence of hypertension and proteinuria, thrombocytopenia, renal insufficiency, liver involvement, cerebral symptoms, or pulmonary edema [2].
Proteinuria is characterized by an abnormal protein excretion and reflects endothelial leakage in preeclampsia syndrome. Overt proteinuria was an essential parameter of the diagnostic criteria and an indicator of the severity of the disease in the past, but it became one of the symptoms for multi-organ involvement because some preeclamptic women may not present or may present with proteinuria at later stage [3]. The following are the criteria of proteinuria for preeclampsia: minimal amount of proteinuria of ≥300 mg/24 hr, a urine protein:creatinine ratio of ≥0.3, or persistent 30 mg/dL (1+ dipstick) protein in random urine samples [2]. Massive proteinuria can develop in some preeclamptic women; although there is no critical definition, it may be defined as urinary protein excretion exceeding 5 g/24 hr [45]. Massive proteinuria has also been removed as a diagnostic criterion for severe preeclampsia because it has a poor correlation with the maternal and fetal outcomes [2]. However, proteinuria, particularly massive proteinuria, is still considered important when we should clinically determine the initial treatment of preeclampsia.
In this study, we investigated whether massive proteinuria in patients diagnosed with preeclampsia is associated with maternal and fetal complications.
Materials and methods
We retrospectively reviewed the clinical records of 233 patients who were diagnosed with preeclampsia and delivered at the Busan Paik Hospital, College of Medicine, Inje University, Korea, between January 2010 and December 2014. The study was approved by the relevant institutional review board of Busan Paik Hospital.
Preeclampsia was defined as gestational hypertension (systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg) arising after 20 weeks of gestation and proteinuria (≥300 mg/day or ≥1+ dipstick) or other adverse conditions. Patients with pre-existing chronic hypertension, previously diagnosed renal or hepatic disease, and thrombocytopenia were excluded.
We divided the preeclampsia patients into three groups based on the amount of proteinuria (massive vs. moderate vs. mild proteinuria group). Massive proteinuria was defined as urinary protein excretion exceeding 5 g in 24 hours. Moderate proteinuria was defined as 2 to 5 g/24 hr and mild proteinuria was defined as <2 g/24 hr. We compared the maternal clinical characteristics, maternal and neonatal complications, and laboratory findings among three groups. Maternal complications included placental abruption, pulmonary edema, pleural effusion, renal insufficiency, hemolysis, elevated liver enzymes, low platelet count (HELLP syndrome, total bilirubin ≥1.2 mg/dL), lactate dehydrogenase >600 IU/L or aspartate aminotransferase >70 IU/L, and platelet count <100 ×109/L), retinal detachment, and eclampsia. Placental abruption was defined as a retroplacental clot detected grossly after delivery. A radiologist determined the presence of pulmonary edema and pleural effusion. Renal insufficiency was defined as serum creatinine concentrations >1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal diseases. Patients with a blurred vision were evaluated by an ophthalmologist using fundoscopy and optical coherence tomography to confirm the retinal detachment. Neonatal complications included 1-minute Apgar score <7, 5-minute Apgar score <7, neonatal death, small for gestational age, jaundice, ventilator care, and seizure. Small for gestational age was defined as the weight below the 10th percentile for gestational age. We evaluated laboratory findings before delivery, including creatinine, aspartate aminotransferase, alanine aminotransferase, albumin levels, and platelet counts.
Data are presented as incidence or mean±standard deviation. Statistical comparisons were performed with one-way analysis of variance for continuous variables and χ2 analysis for categorical variables. Post-hoc pairwise comparisons were performed with SNK (Student-Newman-Keuls) test. Neonatal complications were analyzed using logistic regression. The analysis of neonatal complications was adjusted by gestational age. P-value of <0.05 was considered significant, and the statistical analysis was carried out using MedCalc ver. 11.0 (MedCalc Inc., Mariakerke, Belgium).
Results
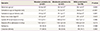
We divided 233 pregnant women into three groups: massive (n=87), moderate (n=67), and mild proteinuria group (n=79). The clinical characteristics of patients are summarized in Table 1. Maternal age was lower in the massive proteinuria group than in the mild proteinuria group (massive group, 32.6±3.8; moderate group, 33.7±4.2; mild group, 34.1±4.4 years; P=0.044). Women in the massive and moderate proteinuria groups had a lower gestational age at diagnosis than those in the mild proteinuria group (massive group, 31.5±3.1; moderate group, 32.3±3.6; mild group, 34.0±3.5 weeks; P<0.001), and a lower gestational age at delivery (massive group, 34.6±3.6; moderate group, 35.1±4.1; mild group, 36.9±4.0 weeks; P=0.001). Body mass index values were lower in the moderate proteinuria group than in the massive and mild proteinuria groups (massive group, 28.5±4.4; moderate group, 27.1±4.0; mild group, 29.1±5.0 kg/m2; P=0.023). Other clinical characteristics, such as systolic blood pressure and diastolic blood pressure at admission, frequency of nulliparity, and cesarean section rate were not significantly different among three groups.
Maternal complications are shown in Table 2. The incidences of pleural effusion and retinal detachment were significantly different among three groups (massive group, 29.9%; moderate group, 22.4%; mild group, 9.0%; P=0.004 for pleural effusion; massive group, 11.5%; moderate group, 3.0%; mild group, 1.3%; P=0.009 for retinal detachment). No significant differences were observed among three groups for other complications, such as placental abruption, pulmonary edema, renal insufficiency, HELLP syndrome, and eclampsia. We analyzed laboratory findings before delivery in the preeclampsia patients. Creatinine levels were significantly higher in the massive proteinuria group than in the moderate and mild groups (massive group, 0.8±0.2; moderate group, 0.7±0.2; mild group, 0.6±0.2 mg/dL; P<0.001), whereas, albumin levels were significantly lower in the massive proteinuria group (massive group, 2.6±0.3; moderate group, 2.8±0.4; mild group, 3.1±0.3 g/dL; P<0.001). Platelet counts were lower in the massive and moderate proteinuria groups than in the mild proteinuria group (massive group, 154.0±73.7; moderate group, 148.2±73.4; mild group, 179.0±65.1 ×109/L; P=0.019). The levels of aspartate aminotransferase and alanine aminotransferase were not statistically significant.
We reviewed the clinical records of 256 babies including 210 singleton pregnancies and 23 twin pregnancies. The neonatal outcomes are presented in Table 3. The frequency of 1-minute Apgar score <7 and ventilator care were statistically significant. But, after adjustment of gestational age, analysis of the frequency of 1-minute Apgar score of <7, 5-minute Apgar score of <7, neonatal death, small for gestational age, jaundice, ventilator care, and seizure showed no significant differences among three groups.
Discussion
Many clinical studies have been conducted to determine the indicators of the severity of preeclampsia, such as blood pressure (≥160 mmHg for systolic blood pressure, or ≥110 mmHg for diastolic blood pressure), massive proteinuria, elevated serum creatinine and transaminase levels, thrombocytopenia, fetal growth restriction, pulmonary edema, and visual disturbance [25678]. Proteinuria, which is a manifestation of widespread renal endothelial damage in preeclampsia, was one of the traditional criteria for the diagnosis of preeclampsia [9]. However, recent clinical research has shown that some women may develop preeclampsia or eclampsia even in the absence of proteinuria, and ignoring these women only because proteinuria has not yet developed may be dangerous for both mother and fetus [3]. Because of this, American College of Obstetricians and Gynecologists task force (2013) widened the spectrum of the diagnosis of preeclampsia to include other criteria, such as thrombocytopenia, renal insufficiency, liver involvement, cerebral symptoms, and pulmonary edema. They also removed massive proteinuria (>5 g/24 hr) as a reliable indicator of the preeclampsia severity [2].
Although massive proteinuria is no longer an essential parameter of severe preeclampsia, we need to consider its association with maternal or neonatal complications in preeclampsia and the associated complications. There have been many studies on the relationship between complications and the amount of proteinuria in preeclampsia. A few studies have reported an increased risk of adverse maternal and fetal outcomes with increasing proteinuria [71011]. According to the recent studies, massive proteinuria could be a marker for early-onset disease, although it was not associated with increased maternal morbidity [12]. Other studies showed that the extent of proteinuria is a poor predictor of either maternal or fetal complications in women with preeclampsia [713]. In our results, preeclampsia occurred earlier in the massive and moderate proteinuria groups than in the mild proteinuria group. Early-onset preeclampsia has been described to occur before 32 to 34 weeks of gestational age and tends to have more severe maternal and fetal outcomes than the late-onset preeclampsia because of the risk of maternal multi-organ dysfunction and fetal mortality [141516]. Gestational age at delivery was also lower in the massive and moderate proteinuria groups than in mild proteinuria group.
Moreover, in our results, massive proteinuria group was significantly associated with some maternal complications, including retinal detachment and plural effusion. In most women with severe preeclampsia, extracellular fluid volume is markedly increased compared with that of normal pregnant women. Vascular endothelial damage with subsequent capillary leakage into the extracellular space is thought to be the main mechanism for increased extracellular volume with intravascular volume depletion in women with preeclampsia [17]. In addition to increased vascular permeability, patients with massive proteinuria have reduced intravascular colloid oncotic pressure with subsequent protein loss. This reduction promotes leakage of fluid from the intravascular compartment into the surrounding interstitium and, theoretically, can lead to a pathological accumulation of fluid in the subretinal space or pleural space. Retinal detachment is a rare complication of preeclampsia, observed in 1% to 2% of the patients with severe preeclampsia [18]. The exact pathophysiology of retinal detachment is not well known; however, choroidal ischemia secondary to accelerated hypertension has been proposed as a cause of preeclampsia [19]. Fluid collection in the subretinal space is related to hydrostatic factors, such as severe acute hypertension [20]. We found that the incidence of retinal detachment was higher in the massive proteinuria group. Pleural effusion in preeclampsia results from low colloid osmotic pressure [21]. In our study, the incidence of pleural effusion was high in the massive proteinuria group that also had a low colloid osmotic pressure. Serum albumin levels were decreased and serum creatinine levels were elevated in the massive proteinuria group, which reflects widespread renal endothelial damage and subsequent loss of albumin. However, massive proteinuria alone was not associated with major complications in women with preeclampsia, such as placental abruption, renal insufficiency, hepatic dysfunction, and eclampsia. Massive proteinuria was not associated with neonatal complications, such as low Apgar score, neonatal death, small for gestational age, jaundice, ventilator care, and seizure.
In conclusion, massive proteinuria might be associated with renal protein excretion-related morbidity, such as pleural effusion, retinal detachment, and low serum albumin levels. Furthermore, massive proteinuria was related to early-onset preeclampsia and early delivery.


 XML Download
XML Download