

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Congenital goiter is an enlarged thyroid gland in newborns, and may be associated with hyperthyroidism, hypothyroidism, or even euthyroidism [1]. Fetal goiter can be caused by several different conditions, including dysgenesis, dyshormonogenesis, maternal ingestion of antithyroid drugs, transplacental passage of maternal antibodies, thyroid stimulating hormone receptor mutation, or tumors [2]. Fetal goiter is a troubling condition because it is associated with a higher rate of neuropathies, serious congenital heart diseases, and even thyroidopathies [1].
Congenital hypothyroidism is very common, affecting about 1:4,000 newborns. The most serious complication of congenital hypothyroidism is the mental retardation, which can usually be avoided if the condition is diagnosed early and treated appropriately. However, even if treatment begins in the first days after birth, newborn infants with clinical characteristics of congenital hypothyroidism may already have suffered substantial damage to the central nervous system [3]. Most cases of fetal goiter are associated with maternal thyroid dysfunction, but there are some reports of this event in euthyroidic pregnant women. These cases are caused by problems in the development of the thyroid resulting from defects in the pathway leading to the synthesis of thyroid hormones. The fetal thyroid gland can be accurately assessed using ultrasound, particularly between 20 and 36 weeks [4]. The diagnosis can be made through ultrasound, by measuring fetal hormones using cordocentesis, and through magnetic resonance imaging (MRI) [1]. Early diagnosis is important to enable early treatment, which can begin during pregnancy [5].
Here, we report a case of fetal goiter identified by ultrasound exam with 34 weeks of gestation. We emphasize the need for early diagnosis, and intrauterine or conservative treatment, in an attempt to reduce or even avoid neurological risks, and above all, to reduce the risk of congenital heart diseases.
Case report
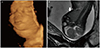
A 41-year-old secundigravida with normal thyroid function, referred with 34 weeks of gestation after ultrasound exam showed a suspected fetal goiter, which proved to be a solid anterior neck mass with uniform vascularization throughout, particularly in the central region (Fig. 1). Three-dimensional ultrasound in rendering mode clearly showed the neck mass. The subsequent ultrasound showed macroglossia and increased cardiac area and amniotic fluid volume. Fetal MRI was conducted and corroborated the diagnosis of goiter (Fig. 2). Cordocentesis was recommended to assess thyroid function and fetal karyotype because of the maternal age and macroglossia, but the parents opted not to perform the invasive procedure. We then opted for conservative management with strict ultrasound monitoring because the findings suggested fetal goiter associated with hyperthyroidism (central vascularization of the mass in color Doppler and early onset of ossification nuclei, as well as cardiac failure). The ultrasound monitoring showed modest increase in the size of neck mass (34 weeks, 66×35×29 mm; 35 weeks, 70×23×35 mm; 37 weeks, 76×30×45 mm), always the vascularization was evident throughout the mass, mainly in the central zone. The cardiothoracic ratio was slightly elevated, ranging from 0.61 to 0.55.
The birth occurred with 38 weeks of gestation by cesarean section. The newborn, a male, weighing 3,445 g, had Apgar scores of 6/8, atypical face shape, and a solid mass in the anterior neck region. The karyotype performed on the umbilical cord blood was normal. The newborn initially had generalized hypotonia, was intubated, and received mechanical ventilation for eight days. Thyroid function tests performed on the second day after birth were normal. Anteroposterior chest X-rays showed slight cardiomegaly. There were no signs of heart failure and no need for vasoactive drugs during hospitalization. The patient's respiratory condition progressively improved, and he was weaned off the mechanical ventilator and then discharged at 22-days-old.
In the early neonatal period (three days) the mass was confirmed by ultrasound exam as an asymmetric goiter and its measurements were 61×40×33 and 45×34×24 mm to the right and left lobes, respectively. At the end of the first month, the respective measurements were the followed: 46×29×37 and 40×33×33 mm to the right and left lobes, respectively. Ultrasound monitoring showed progressive decrease in the size of the thyroid, reaching normal dimensions at six months after delivery. Currently, the infant is one year old, and the function and volume of thyroid gland are normal.
Discussion
Fetal goiter is considered a rare occurrence during intrauterine development, with an incidence of 1:40,000 cases. Fetal thyroid hypertrophy leads to three possible associations: hyperthyroidism, hypothyroidism, and euthyroidism. Consequently, assessment of thyroid hormone function is of great importance for guiding early treatment [1].
The patient in this case was euthyroid, had no family history of the disease, used no medications that regulate thyroid function, and the presence of the fetal goiter was detected. Because the parents opted to not undergo cordocentesis, which is one of the options for assessing fetal thyroid function [6], it was decided to monitor the detailed development of the thyroid gland of the fetus by ultrasound exams. According to Sanz-Cortes et al. [6], ultrasound exam detects the fetal goiter as a homogeneous, symmetrical, and hyperechogenic mass in the anterior neck region, and confirms the condition when the width and circumference of the thyroid gland exceed the 95th percentile for gestational age. MRI complements ultrasound exam to differentiate goiter from other cervical tumors, allowing the assessment of airway obstruction and indication of ex utero intrapartum treatment procedure [78], beyond to contribute to the differentiation of thyroid status: hyperthyroidism from hypothyroidism by analyzing the signals of T1 and T2. In the T2 sequence, the parenchyma signal reduces according to increase the iodine concentration in the gland [9]. In the ultrasound exams performed during our patient's gestation, central vascularization was detected in the fetal thyroid using color Doppler, suggesting it was a case of hyperthyroidism, according to Huel et al. [10].
In a study by Huel et al. [10], the authors mention that in a group of pregnant women who underwent color Doppler examination, peripheral vascularization was detected in 68.8% of the cases involving hypothyroidism, showing that exclusive evaluation of vascularization should not be associated with a specific disorder in the thyroid gland. The presence of characteristics related to vascularization (peripheral/central), heart rate (tachycardia/normal heart rate), fetal movements (intense/normal), and bone maturation (early/late) can guide clinical reasoning, but may not correspond to expectations [10].
The case reported here corresponds to the observations by Huel et al. [10] because central vascularization was verified, indicating possible hyperthyroidism, however the neonate had normal thyroid function. This event, as reported by Jain et al. [11], is rarely described in the literature, since it is common to be reported in hypothyroid fetuses carried by pregnant women with some dysfunction in the thyroid hormones. Ultrasound exam has some advantages, such as facilitating explanation to pregnant women regarding abnormal thyroid size, as well as increasing their adherence to treatment [12]. In this case, the ultrasound exam suggested hyperthyroidism because besides the central vascularization, increased cardiac area was seen along with early onset of fetal ossification nuclei, which facilitated the choice of conduct. On suspicion of hypothyroidism, the assessment of thyroid function for potential intrauterine treatment is essential to avoid long-term neurological outcomes.
In summary, the combination of imaging methods such as ultrasound exam, color Doppler, and MRI is almost a rule when dealing with many fetal diseases such as goiter. Follow-up at a specialist center with a multidisciplinary team and interaction with neonatology professionals, greatly contributed to positive outcomes.

 XML Download
XML Download