

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
An abdominal pregnancy is a rare condition in which the fetus develops in the peritoneal cavity and most abdominal pregnancies may result from tubal or ovarian pregnancies, risk factors are similar to tubal pregnancy with sexually transmitted disease playing a major role [1].
It is believed that abdominal pregnancy is more common in developing countries, but the incidence of abdominal pregnancy also appears to be increasing recently in developed countries due to the growing use of assisted reproductive technology [2] and cocaine abuse [3]. The maternal mortality rate can be as high as 20% [4], 7.7 times that of tubal pregnancy and 90 times that of intrauterine pregnancy [1]. This is primarily because of the risk of massive hemorrhage from partial and total placental separation. Accurate localization of the placenta preoperatively could minimize blood loss during surgery. The perinatal mortality is in the range 40% to 95%, and between 20% and 90% of the surviving fetuses have serious malformations due to compression (lack of the amniotic fluid buffer and the absence of the uterine wall) and vascular disruption [5].
Abdominal pregnancy is classified as primary or secondary. According to Studdiford’s criteria [6] the diagnosis of primary abdominal pregnancy is based on the following anatomic conditions: (1) normal bilateral tubes and ovaries, (2) absence of an uteroplacental fistula, and (3) attachment exclusively to a peritoneal surface early enough in gestation to eliminate the likelihood of secondary implantation. Secondary abdominal pregnancies are most common and are mostly a result of tubal abortion or early rupture of tubal pregnancy with subsequent reimplantation of the conceptus in the peritoneal cavity. Since we had a difficult time finding related publications on abdominal pregnancy in human immunodeficiency virus (HIV) positive woman, we present our unusual case discovered during the capacity building program in Dar es Salaam, Tanzania.
Case report
On July 23rd 2015, a 27-year-old gravida 3, para 2 woman with a 2-week history of intermittent abdominal pain, especially aggravated during sexual intercourse, was referred to Amana Regional Referral Hospital in Dar es Salaam. The patient was amenorrheic for 4 months and had last normal vaginal delivery 7 years ago. Vital signs and initial laboratory parameters were nomal. On physical examination, her abdomen was distended with a fundal height corresponding to approximately 20 weeks, which distends more than it should. Vaginal examination showed the presence of a single cervix. She had been irregularly using oral contraceptive pills after her second pregnancy, and had a history of sexual transmitted infection in December 2014.
In June 2015, she was diagnosed with HIV and started antiretroviral therapy. Her HIV regimen includes Atripla and Septrin for opportunistic infections. For accurate diagnosis an ultrasound examination was thus performed. Transabdominal sonography revealed a single live fetus appearing to be extrauterine with transverse lie, which is very close to the anterior abdominal wall. The fetal biparietal diameter of 2.6 cm and crown-rump length of 6.7 cm were measured and corresponded to the 13+ weeks mean and fetal cardiac activity was over 100 beats/min. There was no demonstrable uterine myometrium around the fetus and cramped fetal parts with reduced to no amniotic fluid (Fig. 1). Because an empty uterus can easily be missed on a routine transabdominal ultrasound scan, transvaginal ultrasound scan was used for clearer visualization of the uterine cavity. Transvaginal ultrasound scan revealed an empty uterus and a moderate amount of free fluid in the Pouch of Douglas.
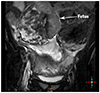
On July 27th 2015, to confirm the presumptive diagnosis of abdominal pregnancy, a subsequent abdomen-pelvis magnetic resonance imaging was performed at Muhimbili National Hospital in Dar es Salaam, and it showed no intrauterine gestational sac while a fetus was visualized in right abdomen with the placenta in the right iliac fossa (Fig. 2).
On July 29th 2015, the patient suddenly developed intensified abdominal pain, her blood pressure fell to 80/40 mmHg and hemoglobin of 6.5 g/dL. Emergency laparotomy was performed. Under general anesthesia, a midline incision above the umbilicus was made. On opening the abdomen, about 1,500 mL of blood associated with clots was found and removed from the peritoneal cavity. The placenta was attached between the anterior and posterior leaves of right broad ligament and also implanted over right adnexal and ileocolic region. The right fallopian tube and ovary were severely distorted which is highly suggestive of a tubal pregnancy that ruptured and resulted in secondary implantation in the peritoneal cavity, and they were neither well visible because of extensive pelvic adhesion. The left fallopian tube and ovary were normal. The uterus was found to be empty and small.
A gestational sac lying on the right side of the abdominal cavity superior to the uterus was seen and part of the fetus was protruding from it. The gestational sac was incised, the fetus was extracted, and the umbilical cord was clamped and ligated at its base. Large portions of placenta were adhered to segments of the large bowel, omentum, and right adnexal region of the uterus and there was significant bleeding from the partially detached placenta, which prompted removal of about 80% of the placenta to facilitate hemostasis. The rest of the placenta was left in situ. Unilateral adnexectomy and partial omentectomy were also performed. One unit of blood was transfused intraoperatively and another unit of blood was given postoperatively. The patient recovered without any other complications and was released from hospital on the 5th postoperative day, and no abnormality was detected on subsequent ultrasound examination.
On November 16th 2015, the patient tested for CD4 count and the result was 502 cells/mm3, a good sign that antiretroviral therapy is working effectively. On December 4th 2015, 4 months after the termination of pregnancy, she also tested for beta-human chorionic gonadotropin and the level had completely regressed to less than 1 mIU/mL.
Discussion
The clinical symptoms of an uncomplicated abdominal pregnancy are rather unspecific and about up to 60% of abdominal pregnancies are missed at the time of initial presentation, and can go undetected until an advanced gestational age and often result in massive hemorrhage [7]. Many times it only has been discovered after failed induction of labor or upon laparotomy [58].
Use of transvaginal ultrasound scan is superior to transabdominal ultrasound scan in the evaluation of early abdominal pregnancy since it allows a better view of the adnexa and uterine cavity [4]. As in our case, the sonographic findings suggestive of abdominal pregnancy include the appearance of an empty uterus, absence of a myometrium around the fetus or absence of myometrial tissue between the bladder and the gestational sac, relative oligohydramnios, the fetal parts being very close to the abdominal wall, an abnormal lie, poor visualization of the placenta, and free intra-abdominal fluid [9].
As a separate uterus was identified away from the fetus, the possibilities of pregnancy in a uterus didelphys or a bicornuate uterus pregnancy (the empty uterine cavity was mistaken for the empty horn) were also considered [5]. Magnetic resonance imaging is complementary imaging modality that helps not only to confirm the diagnosis but also allows the precise anatomical location of the fetus and placenta. Because of the high risk of maternal complications due to placental separation and the poor prognosis for the fetus if the pregnancy continues, surgical intervention is recommended as soon as the diagnosis of abdominal pregnancy is confirmed, regardless of gestational age or fetal condition [1]. Management by laparotomy is preferred, particularly when there is a high risk of hemorrhage.
For the management of placenta, whenever safely possible, the removal of the placenta is a rule. However, most of times the placenta in abdominal pregnancy is located over tissue that cannot contract and attempts of its removal may lead to massive hemorrhage. There are also other treatment options regarding the placenta, like partial removal or leaving the placenta in situ. In case of a partial removal of the placenta, there is a need to follow up the patient with beta-human chorionic gonadotropin level for evidence of placental absorption.
In our case, the co-existence of HIV and abdominal pregnancy raises specific management dilemmas: the increased risk of bleeding if attempts are made to remove the placenta in immune-compromised woman, and the risk of infection if the placenta is left in situ. We decided to remove most of the placenta, and the placenta was meticulously separated and a complete hemostasis was achieved.
In conclusion, the diagnosis of abdominal pregnancy is often missed even with routine ultrasonographic examination and is even more difficult if the pregnancy is advanced, awareness of this condition is very important. Despite overall improvements in ultrasound, still the incidence of the diagnostic error is very high. More emphasis should be placed on strengthening the capacity of clinicians, especially in developing countries where the ultrasound has only recently been introduced.
It is vital for the diagnosis of abdominal pregnancy to be made early in pregnancy and prompt intervention taken to prevent life-threatening complications. Removal of the placental tissue is less difficult in early pregnancy as it is likely to be smaller and less vascular.

 XML Download
XML Download