

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Neuroendocrine cervical carcinoma (NECC) is a rare form of cervical cancer representing 0.5% to 5% of all cervical cancer cases. NECC is classified into four histologic subtypes (small cell, large, classical carcinoid and atypical carcinoid, with small cell carcinoma of cervix (SCCC) being the most frequent type [1]. Neuroendocrine carcinomas can be identified by characteristic light and electron microscopic criteria, such as small cells with hyperchromatic nuclei and scanty cytoplasm. NECC can be present with other histologic findings, such as squamous cell and adenocarcinoma, and the presence of the NECC component defines the clinical behavior [2].
The clinical course of SCCC is aggressive, and metastasis to the bone, brain, liver, and bone marrow is common [3]. The relapse and metastasis pattern infers the nature of hematogenous dissemination [4]. Despite its known clinical behavior, there is no consistent method of treatment. The treatment regimen is based on small cell lung cancer, where the microscopic characteristics are similar. This regimen is also applied to other types of NECC. Interestingly, Hoskins et al. [5] reported a three-year failure-free survival rate of 80% in early stages (I to II) patients who received primary radiation therapy and platinum-based combination chemotherapy. A recent study showed that primary radiation therapy with at least 5 cycles of platinum-based chemotherapy resulted in a five-year overall survival rate of 78%, better than that of 46% achieved through primary surgery alone in early stage SCCC [6]. However, some studies have reported primary radical surgery followed by adjuvant chemotherapy as the preferred treatment modality with relatively favorable survival outcomes [7].
Due to the low incidence of NECC, it is very difficult to undertake prospective studies to elucidate the impact of treatment modality on survival outcome. Moreover according to our review, there are not enough studies with sufficient cases in the Korean population. Thus, to understand the prognosis in our population and improve the treatment strategy, we evaluated the clinical and pathologic factors associated with survival in patients with NECC in two of the cancer institutes in Korea.
Materials and methods
Patients diagnosed with NECC and treated between 2000 and 2014 at Seoul National University Hospital and the National Cancer Center were included in the study. One case of a patient who died due to sepsis caused by aggravating myelodysplastic syndrome was excluded. Clinicopathologic data were collected from hospital charts and scanned records. Staging was done based on International Federation of Gynecology and Obstetrics (FIGO) clinical staging criteria. Early stage was defined as stage I to IIA and advanced stage was as stages IIB and above. All patients underwent physical examination, imaging study (pelvic computed tomography, chest computed tomography and pelvic magnetic resonance imaging if indicated), intravenous pyelography, and cystoscopy. Patients with tumors confined to the cervix typically underwent radical hysterectomy with pelvic lymphadenectomy. For advanced cases, radiotherapy with or without chemotherapy was performed. Adjuvant therapy using chemotherapy or concurrent chemoradiation therapy (CCRT) was carried out except for in one case of stage 1B1. The association between risk factors and prognosis was evaluated using Kaplan-Meier survival analyses and log-rank tests. The independent factors found to be predictive of survival were evaluated using Cox regression methods. P-values <0.05 were considered significant. All analyses were performed using PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA) and MedCalc ver. 15.8 (MedCalc Software bvba., Acacialaan, Ostend, Belgium). The institutional review board approval number for this study is 1507-013-686.
Results
A total of 61 patients were diagnosed and treated in this study. The median age was 49 years (range, 28 to 74), and 41 patients had early-stage (I to IIA) disease. Patients' demographic and clinicopathologic characteristics are shown in Table 1. Small cell carcinoma was the most common histologic type, comprising 67.2% of the cases. Among early-stage patients treated by radical hysterectomy, lymphovascular space invasion was found in 19 cases (59.3%). By immunohistochemistry, the three types of neuroendocrine marker (synaptophysin, chromogranin, and CD 56) were stained with similar frequency.
Tables 2 and 3 show the treatment methods of the 61 patients. Of the early-stage patients, 32 (78%) underwent radical hysterectomy as a primary treatment. Among them, 22 (68.8%) patients underwent pelvic lymph node dissection and of those, eight patients underwent additional para-aortic lymph node dissection. Adjuvant therapy using chemotherapy or CCRT was conducted in most (31/32) cases. There was no specific difference in median survival between chemotherapy and CCRT. For advanced-stage patients, the main treatment modalities were chemotherapy (60%) and CCRT (25%). There was no significant difference in prognosis between the two groups. Two patients underwent primary surgery. One stage IIB patient underwent pelvic exenteration and another stage IIB patient underwent pelvic and para-aortic lymph node dissection before CCRT.
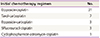
Post-treatment surveillance was conducted every three months. For patients experiencing recurrence, radiation and/or chemotherapy were employed. As a first-line chemotherapeutic agent, etoposide was used most frequently (Table 3). The efficacy of the different regimens was not clearly proved in this study.
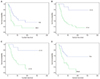
We evaluated the significance of various clinical factors that may influence the prognosis and overall survival (Table 4, Fig. 1). Early-stage patients had a median survival time of 77 months compared with 40 months in the advanced-stage group (P=0.013). The estimated five-year survival rate was 42.1% for early-stage patients and 23.7% for advanced-stage patients. In all cases, patients with tumor size ≥2 cm had a median survival time of 47 months compared with 133 months in those with tumor size <2 cm. To remove the stage factor, a subgroup analysis on the early-stage group was done. Early-stage patients with tumor size ≥2 cm had a median survival time of 44 months compared with 130 months in the group with tumor size <2 cm. Other pathologic factors that may influence prognosis (e.g., residual tumor, tumor homology, lymph node involvement, lymphovascular space invasion, neuroendocrine markers) were also evaluated. In all of the radical hysterectomy cases, the resection margin was free from carcinoma. Of the histologic factors, only mixed histology proved to be a poor prognostic factor (P=0.004). Age had no significant effect on survival. All the preceding factors were re-evaluated only in small cell neuroendocrine carcinoma subtype cases and the statistical results were similar with identical prognosis factors. In the multivariate analysis, tumor stage, tumor size and tumor homology proved to be significant independent prognostic factors. Immunohistochemical analysis was performed in 43 of 61 cases. In the remaining 18 cases, only microscopic diagnosis was performed. Thus, subgroup analysis was performed particularly in immunohistochemically confirmed cases and the statistical results were similar.
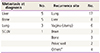
Sites of metastasis at diagnosis and frequent recurrence sites after initial treatment are shown in Table 5. Major primary metastatic sites were the liver and bone. Tumor recurrence was found in 39.3% of all patients. Despite the large earlystage group, the recurrence rate was 51.2%. Main sites of distant recurrence were the lung and liver.
Discussion
NECC is a rare form of cervical carcinoma and consequently, prospective randomized trials to evaluate the impact of different treatments on patient outcome have not been possible. In recent years, novel NECC treatment methods have attempted to replicate successful treatments for small cell lung carcinoma. Currently, surgical resection only plays a limited role in patients with early-stage small cell lung cancer [8]. Moreover, a report has suggested that radical hysterectomy does not prolong the survival of SCCC patients [5]. However, our results showed that radical surgery is an important component in the multimodal treatment of NECC. The survival rate in this study was better than that in previous studies. For example, Cohen et al. [9] previously analyzed the survival outcomes of 188 patients from 1979 to 2005 and found the estimated five-year survival rate to be 36.8% for early-stage patients and only 8.9% for advanced-stage patients. In our study, the rates were 42.1% and 23.7% respectively. Some factors may have contributed to the improvement of survival. First, in all surgical cases the resection margin was free from cancer. Improved surgical skills and the use of frozen section examination during the surgery may have contributed to this progression. Second, Deacon et al. [10] and Chan et al. [11] have suggested smoking as a poor prognostic factor in cervical cancer and SCCC respectively. In our case, there were only two patients with history of smoking and that may be attributed to the low female smoking rate in the Korean population. Third, due to the limited randomized controlled clinical trial for NECC, some therapeutic guidelines (e.g., multimodality therapy on early-stage patients, using etoposide-containing chemotherapeutic regimens) were suggested [912]. These may have led to the improved outcome.
Several studies have reported disease stage as the strongest predictor of outcome, and that other factors (age, tumor size, depth of stromal invasion, and vascular space invasion) as prognostic factors in SCCC [7]. However, in our study, FIGO stage, tumor size, and tumor homology were independent prognostic factors of survival, and our univariate and multivariate analyses found no association between age, depth of stromal invasion, or vascular space invasion and NECC patient outcome. In a previous study, patients with a mixed histologic pattern had a better prognosis than those with a homogenous pettern [11]. However, others found no relationship between tissue homology and prognosis [1213]. In our study, patients with a homogenous histologic pattern had a better prognosis, but racial and etiologic differences (e.g., low smoking rates, human papillomavirus infection) may be confounding factors, and further studies with more cases are required to clarify this correlation.
A previous study reported the effectiveness of etoposide with platinum-based chemotherapy for NECC but not for well-differentiated carcinoid tumors [2]. Chang et al. [12] found that chemotherapies containing cisplatin and etoposide could be effective in patients with early-stage SCCC following radical hysterectomy. A recent study showed that platinum-based combination chemotherapy was an independent prognostic factor for improved survival in patients with SCCC [14]. In our current study, there were no prognostic differences between etoposide and other regimens. More well-designed case-control studies are needed to verify effect of the regimen. The overall tumor recurrence rate was 39.3%, and the early-stage recurrence rate was as high as 51.2%. Because of the limited number of patients in our study, we could not detect a significant survival benefit in patients who received adjuvant chemotherapy. However, considering the features of early recurrence and distant metastasis with NECC, it is likely that adjuvant chemotherapy would enhance survival relative to radiation alone.
In conclusion, tumor stage and tumor size may act as surrogates for factors prognostic of survival in patients with NECC. Moreover, our results indicate that primary radical surgery followed by adjuvant chemotherapy may be the preferred treatment modality for patients with early-stage NECC.



 XML Download
XML Download