

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Epignathus or oral teratoma is an extremely rare congenital tumor, which arises in the sphenoid region of the palate or pharynx, occurring in 1 in 35,000 to 1 in 200,000 live births [1]. The tumor fills the oral cavity and hence is associated with a high mortality rate owing to severe airway obstruction, especially in the neonatal period [1,2,3]. Usually, this tumor was detected in late second trimester or third trimester [2,3], but technical developments in three-dimensional (3D) ultrasonography and magnetic resonance imaging (MRI) have enabled early diagnosis and detailed characterization of the tumor [4,5,6]. Herein, we present a case of epignathus affecting 1 fetus in a twin pregnancy. The epignathus in this case was associated with multiple congenital malformation including cleft palate, bifid tongue, bifid uvula, congenital heart defect, and bilateral inguinal hernias. To the best of our knowledge, this constellation of congenital malformations has not been reported previously. In addition, we examined the clinical value of 3D ultrasound and MRI during antenatal counseling and the establishment of peripartum management.
Case report
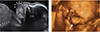
A 28-year-old woman pregnant with twins was transferred to our institution for abnormal findings on ultrasonography in one twin's oral cavity at 20 weeks 6/7 days of gestation. In a 2D sonogram, one fetus in the dichorionic-diamniotic twin pregnancy had a solid and cystic mass measuring 13×9 mm that originated in the mouth, extended outside the mouth, and showed no vascularization on color Doppler examination. Using 3D ultrasonography in surface-rendering mode, we confirmed the presence of an oral tumor, distinguishable from the lips (Fig. 1). Then, using the 3D sonogram, we explained the perinatal risks related to airway obstruction caused by the fetal lesion to the mother and her family. She required further antenatal work-up for precise delineation of the mass and further counseling regarding whether the mass could be resected after delivery. She refused to undergo anantenatal chromosomal test because of the risk to the other twin through amniocentesis.
To examine the relationship between the tumor and surrounding structures, we performed a fetal MRI. A sagittal HASTE T2-weighted MRI scan showed a hyperintense mass with a stalk projecting from the palate and upper lip, measuring 16×10 mm in size in the lower-positioned fetus. There was no evidence of central nervous system, CNS-related anomaly and intracranial invasion of the tumor. A multidisciplinary medical team comprising an obstetrician, otolaryngologist, neonatologist, and radiologist discussed the diagnosis and management of the tumor; they planned to perform elective surgery after birth rather than the ex utero intrapartum treatment (EXIT) procedure, considering that endotracheal intubation of the newborn would be possible after birth according to the fetal MRI scan.
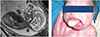
The size of the lesion had increased to 22×17 mm at 32 weeks of gestation. Swallowing difficulty and polyhydramnios were not noted. At 33 weeks 5/7 days of gestation, an emergency cesarean section was performed because of premature rupture of the amniotic membrane. The male neonate weighing 1,745 g with the oral mass was delivered first; his Apgar scores were 5 at 1 minute and 6 at 5 minutes. The neonate was immediately endotracheally intubated. The oral mass was whitish, soft, and movable, and measured approximately 20×25 mm (Fig. 2A). It appeared to originate from the hard palate and a fibrous band was observed between the mass and the tongue base. The mass was accompanied by complete cleft palate, bifid uvula, and bifid tongue. Bilateral inguinal hernias were also found on physical examination. Moreover, a small ventricular septal defect and patent ductus arteriosus were observed on echocardiography. The chromosome analysis of the affected neonate showed normal karyotype (46, XY). The second baby weighing 2,090 g had no gross anomaly. At 10 days after birth, the tumor was excised and the tongue was reconstructed (Fig. 2B). The resected tissue measured 40×23 mm and microscopic examination showed the presence of some hair follicles with mature adipocytes and keratinized squamous epithelium, consistent with mature teratoma. A bilateral inguinal herniotomy was performed on day 73 at the age of 13 months; the baby's condition was good.
Discussion
Epignathus is known to be associated with other malformations in 6% of all epignathus cases [3,7]. Cleft palate is the most common malformation, as the tumor prevents closure of the palate [7]. Other associated malformations are bifid tongue or nose, glossoptosis, diaphragmatic hernia, nasopharyngeal teratoma, and an inguinal hernia [7,8]. Bifidity and glossoptosis indicate impaired fusion of the primitive tongue buds and anterior positioning of the tongue because of very early development of the tumor. Moreover, functional disorders secondary to glossoptosis can also hinder the growth of the jaw, resulting in mandibular microretrognathia. The case presented here was that of epignathus accompanied by multiple malformations, a cleft palate, bifid tongue, bifid uvula, congenital heart defects, and bilateral inguinal hernias, without chromosomal defect.
In some studies, epignathi have been found to be associated with chromosomal abnormalities, early embryonic defects, or fetal syndrome [7,9,10]; however, to the best of our knowledge, no study in the literature has reported recurrent fetal epignathus.
Epignathus can present in a variety of ways. High levels of maternal serum α-fetoprotein indicate the presence of a tumor that can be confirmed by ultrasonography [10]. Epignathus could also be identified by 2D ultrasonography, as seen in this case. The antenatal finding of epignathus is an anterior or bidirectional organoid facial mass, which is partially solid and cystic [4]. Polyhydramnios occurs in approximately 30% of the cases, secondary to obstruction of the mouth of the fetus and swallowing difficulty because of the local mass [7,11,12]. In the case presented here, polyhydramnios was not found, probably because of the relatively small size of the intraoral stalk part of the tumor, and partially accompanying cleft palate.
3D ultrasonography could facilitate prenatal diagnosis and help in planning delivery, through the various 3D software programs such as the surface-rendering mode, the "multislice" view, the "reverse face" view, and tomographic mode [4,5,6]. Reconstructed images from the 3D volume data can provide information about the size, location, composition, and extension of the tumor. The resolution is limited, however, when examining the intraoral mass [6]. In the case discussed here, we used 3D ultrasonography in the surface-rendering mode, and the resultant sonograms were used to explain to the patient what fetal lesions are, but they were not very helpful in revealing any anatomical relationship of the lesion with the surrounding tissues because of the interference of the other twin and perioral structures.
Fetal MRI, a complementary diagnostic tool for epignathus [13], might be especially useful in identifying the need for an EXIT procedure to be performed on a fetus. MRI is helpful in ensuring airway patency by establishing a relationship between the mass and airway structures. In addition, this modality is useful in the assessment of the intracranial invasion that contributes to the poor prognosis of the patients. In this case, we were able to view an enhanced characterization of the tumor and ensure airway patency of the fetus through the MRI scans, which informed peripartum management.
If tracheal obstruction is prenatally suspected, physicians should consider a cesarean section and subsequent intubation by tracheostomy before the umbilical cord is clamped, as prescribed in the EXIT procedure, or resection of the tumor mass while the newborn is on placental support [7]. Immediate intubation and oxygenation, however, might fail because of the huge size of the tumor, and surgical removal is difficult owing to modification of anatomical landmarks [3,14]. Some authors have suggested that a short EXIT procedure limited to securing the airway of the fetus followed by early surgery is preferable to confirmative resection under placental support [15].
Prognosis depends on the size and location of the tumor, the rate of growth, associated polyhydramnios, and the degree of intracranial spread [7]. Malignant degeneration rarely occurs in cases of epignathus teratoma. Polyhydramnios, commonly caused by swallowing difficulties, is an important factor for prognosis because it indicates the severity of airway obstruction and the extent of tumor invasion; polyhydramnios is also associated with an increased risk of preterm labor, preterm premature rupture of membranes and further pulmonary hypoplasia, and respiratory distress in the neonate.
In conclusion, this report described the case of a single twin with epignathus associated with inguinal hernia and other malformations. According to the studies in the related literature, although the images reconstructed from the 3D ultrasonography data are valuable in the diagnosis of tumors of the head and neck, the usefulness of these data were limited in the case herein because of low resolution. Fetal MRI helped determine if special management of the tumor was necessary for securing the airway.
 XML Download
XML Download