

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Radical trachelectomy is a promising fertility-preserving procedure for early stage cervical cancer [1]. However, isthmic stenosis occurs in around 15% of patients who received radical trachelectomy and it is a major cause of infertility following radical trachelectomy [2]. Moreover, despite the treatment for recanalization of isthmic stenosis, recanalization often fails or isthmic stenosis sometimes recurs. We report a successful pregnancy and child-birth following direct intraperitoneal insemination (DIPI) in an infertile patient with failure of dilatation and recanalization of isthmic stenosis occurred after laparoscopic radical trachelectomy.
Case report
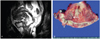
On July 2006, a 32-year-old nulligravida had a laparoscopic radical trachelectomy with pelvic and paraaortic lymph node dissection due to cervical cancer IB1. The tumor size was less than 3.3 cm and pathology was confirmed as poorly differentiated squamous cell carcinoma with clear resection margin (Fig. 1). There were no postoperative complications and any adjuvant treatment was not given after operation.
In 2009, she visited our hospital due to amenorrhea for 6 months. Her serum follicle-stimulating hormone and estradiol concentrations were within the normal ranges with 8.1 mIU/mL and 210 pg/mL, respectively. Ultrasonography (USG)-guided sounding was performed for estimating isthmic patency and isthmic stenosis was confirmed. She wished to be pregnant and therefore she was referred to our infertility clinic. Routine work-up for infertility was performed. All laboratory tests including semen analysis showed normal results. We performed an USG-guided dilatation of isthmovaginal opening, nonetheless isthmovaginal recanalization failed. On August 2009, reconstruction of isthmovaginal opening and isthmovaginal anastomosis were performed again to solve this problem under general anesthesia. On the next month, intrauterine insemination (IUI) was performed during controlled ovarian stimulation (COS) cycle using gonadotropin releasing hormone (GnRH) antagonist multiple dose protocol (MDP) but she failed to become pregnant.
On January 2010, patient visited our infertility clinic for second cycle of IUI. Unfortunately, we found isthmic restenosis and decided to try DIPI after consultation with patient. On Feburary 2010, DIPI was performed under transvaginal (TV) USG guidance during COS cycle using GnRH antagonist MDP but patient failed to become pregnant. Although we performed second cycle of intraperitoneal insemination (IPI) during COS cycle using GnRH antagonist MDP on July 2010, patient also failed to get pregnant. On October 2010, DIPI in natural ovulatory cycle was performed again. When dominant follicle reached a mean diameter of 18 mm, a recombinant human chorionic gonadotropin (rhCG, Ovidrel, Merck Serono SA, Geneva, Switzerland) of 250 µg was administered subcutaneously to trigger follicular maturation. DIPI was performed 36 hours after rhCG injection. For DIPI, partner's semen was obtained by masturbation and liquefied at room temperature and then its amount, sperm concentration, and sperm motility were evaluated. Partner's sperm concentration was 214×106/mL and percentages of motile sperm and sperm with normal morphology were 61% and 23%, respectively. Semen was layered upon a dual-density gradient (Ception, Sage international, Trumbull, CT, USA) and centrifuged at 300 g for 20 minutes and then washed again with Quinn's sperm washing media (Sage international) by centrifugation at 300 g for 10 minutes. The vagina was cleansed and TV USG was performed to identify the fluid in the posterior cul-de-sac (PCDS) and ovaries. A 30 cm long 17 gauge disposable needle (Cook, Bloomington, IN, USA) was placed in a needle guide attached to the vaginal probe. The needle was put into the PCDS along the biopsy guide. The syringe containing the prepared semen sample is attached to the needle and the semen sample of 2 mL was injected directly into the PCDS (Fig. 2). Intravenous sedation was not carried out during DIPI. Luteal support was provided by administering 90 mg of vaginal progesterone gel (Crinone gel 8%, Merck Serono SA) once daily from the day of DIPI. Pregnancies were confirmed by rising serum β-human chorionic gonadotropin (β-hCG) concentrations and transvaginal ultrasonographic evidence of a gestational sac. Luteal support was commenced with 400 mg/day transvaginal progesterone insertion from the day of IPI. A serum β-hCG measured 20 days after DIPI was 2,660 mIU/mL and on the same day, a gestational sac with a mean diameter of 2.4 mm was visualized in TV USG. The intrapartum course was uncomplicated though whole pregnancy period. An amniocentesis for fetal karyotyping which was performed at 15 weeks of gestation showed normal results. Classical Ceasarean section was performed due to previous laparoscopic radical trachelectomy and T-lie presentation at 37 weeks of gestation and 3,330 g female baby was born and her Apgar score at 1 and 3 minutes after birth were 7 and 9. Both uterine artery embolization was performed after Cesarean section due to postpartum heavy uterine bleeding and then emergency transabdominal hysterectomy was performed due to persistent bleeding despite uterine artery embolization. On postoperative 15th day, she was discharged in good health.
Discussion
It is estimated that 43% of all cases of cervical carcinoma in the USA were diagnosed in women younger than 45 years of age in 2004 [3]. Additionally, 10% to 15% of cases of cervical cancer are diagnosed during the childbearing years [4]. Recently, women often delay childbearing even until the mid to late 30s and this can result in the increase of incidence of cervical cancer during the childbearing years. For selected patients with stage I cervical cancer who want to preserve her fertility, radical trachelectomy has emerged as a reasonable fertility-sparing operation.
There are some concerns regarding pregnancy in patients on whom radical trachelectomy was performed. First, conception may be difficult in these patients due to decreased cervical mucus, isthmic stenosis, and surgical adhesions. Actually, it was reported that 75% of the infertility after trachelectomy was caused by cervical factor [5]. Boss et al. [2] reported that the incidence of infertility and isthmic stenosis after radical trachelectomy were 25% to 30% and 15%, respectively. Isthmic stenosis still remains a challenge as to the problem of cannulating the isthmus for embryo transfer (ET) or IUI. Isthmic stenosis can lead to not only infertility but also menstrual disorder, hematometra and abdominal cramp. Isthmic dilatation is the solution for this problem and this procedure may need to be repeated in-between treatments. Despite the Isthmic dilatation, recanalization of isthmic stenosis often fails. Even after successful treatment of isthmic stenosis, isthmic stenosis sometimes recurs. If isthmic dilatation succeeds and isthmovaginal patency is obtained, IUI is the best and most cost effective choice in patients with patent fallopian tubes and/or mild male factor infertility. However, when isthmovaginal patency is not obtained, reproductive physician should try alternative procedure. In this case, we firstly performed a reconstruction of isthmovaginal opening and isthmic dilatation for treatment of isthmic stenosis. Nevertheless, patient suffered from recurred isthmic stenosis. In this condition, transcervical access is impossible and therefore, transmyometrial ET has been used with some success. In 1993, Kato et al. [6] reported 38 cases of successful TV-transmyometrial embryonic transfer among 104 patients with cervical factor infertility. However, if patients do not have other infertility factor except cervical factor, transmyometrial ET is not suitable as a first line treatment for them. Transmyometrial ET is time and cost consuming procedure and also likely to produce considerable endometrial trauma. Therefore, transmyometrial ET should be considered as a last resort [7].
DIPI can be chosen as a first line treatment in patients with unsolved or recurrent isthmic stenosis where tubal patency has been confirmed, no intrauteriune contour defects exist, and there is no profound male factor infertility [8-10]. Previous randomized study comparing pregnancy rates after IPI and standard IUI showed roughly equivalent outcomes [10]. DIPI can be a possible alternative to surgical ET in patients with failure of recanalization of isthmic stenosis happened after radical trachelectomy. However, it is hard to find reports or literatures regarding DIPI attempted in infertile patients with isthmic stenosis following radical trachelectomy. Therefore, we report a successful pregnancy and birth by DIPI in an infertile woman with failure of recanalization of isthmic stenosis following laparoscopic radical trachelectomy.

 XML Download
XML Download