

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With the gradual increase of the life expectancy of women, the prevalence of women with pelvic organ prolapse (POP) is increasing, and 40.8% of postmenopausal women aged 50 to 79 years who enrolled in the Women's Health Initiative Hormone Replacement Therapy Clinical Trial [1] have been reported to have some degree of POP.
POP is regarded as an abnormal descent or herniation of the pelvic organs, including the uterus, anterior and posterior vagina, bladder, urethra, and rectum, from their normal anatomical position in the pelvis, which is caused by the weakness of the pelvic floor muscle and the connective tissue. Advanced POP is often noted to be related with the presence of lower urinary tract dysfunction, such as bladder outlet obstruction (BOO), urinary incontinence (UI), and detrusor dysfunction [2].
BOO is caused by urethral compression when co-existing with not only apical but also posterior as well as anterior compartment prolapsed [3]. Prolapse of the bladder or urethra and the mechanical obstruction of the urinary system caused by uterine prolapse can lead to increased urinary resistance, incomplete bladder emptying, and secondary changes in the detrusor [4]. Patients with POP have a higher incidence of bladder trabeculation, which is the secondary result of BOO and is caused by morphological and histological changes due to hypertrophy and hyperplasia of the bladder muscle, as found in other studies [4-8].
There have been few objective studies on female BOO and its related symptoms and diagnosis. Some studies have demonstrated that half of all women with POP have a feeling of incomplete bladder emptying, but only 30% of the patients with advanced POP have urodynamic evidence of BOO [9,10]. Some studies tried to suggest an association between BOO and bladder trabeculation in stress urinary incontinence (SUI) patients, but there are no objective evidences of such.
The aim of this study was to determine the significance of BOO in preoperative urodynamic studies (UDS) in women who had been diagnosed with pelvic floor dysfunction, including POP and SUI. The relationship between BOO and bladder trabeculation in patients with POP and SUI was demonstrated.
Materials and methods
After approval of the Severance Hospital Institutional Review Board Committee, the medical records of 150 patients who had been diagnosed with pelvic floor dysfunction and who underwent preoperative UDS at Yonsei University Health System within the period from January 2006 to March 2012 were reviewed. The patients were divided into two groups: a group of 50 patients with BOO and a group of 100 patients without BOO in the preoperative UDS. Among the 50 patients with BOO, there were 25 patients who had been diagnosed with POP-with-SUI and 25 patients who had been diagnosed with SUI only. Among the 100 patients without BOO, there were 50 patients who had been diagnosed with POP-with-SUI and 50 patients who had been diagnosed with SUI only. All the women provided their medical and gynecologic histories and underwent cystoscopy, and UDS was performed after restoration of the prolapsed organ by the same examiner. POP surgery and a combination of procedures were performed by an experienced surgeon in the authors' institution after an accomplished informed consent form was obtained from each patient.
A suspicious BOO was determined as a maximal flow rate in free-flow study (Qmax) less than 12 mL/sec and a detrusor pressure at Qmax in pressure-flow study (PdetQmax) higher than 20 cmH2O in the UDS [11]. The patients with and without BOO were compared in a preoperative UDS, and their baseline demographics, including their age, body mass index (BMI), presence of menopause, history of pelvic surgery, and presence of difficult labor, were reviewed retrospectively. The parameters of the UDS, such as Qmax (mL/sec), PdetQmax (cmH2O), postvoidal residual volume (PVR, mL), maximal cystometric capacity (MCC, mL), valsalva leak point pressure (VLPP), maximum urethra closure pressure (MUCP), and prevalence of detrusor overactivity (DO), were evaluated. The preoperative and postoperative urinary symptoms, including frequency, urgency, stress incontinence, urgency incontinence, dysuria, and urinary retention, were also assessed, using urogenital distress inventory-6 (UDI-6) (Fig. 1) [12]. UDI-6 consists of six questionnaires evaluating the subjective improvement of the urinary symptoms. The UDI-6 form has a value between 0 and 3, according to how much the patient is bothered by each symptom, whereas in this study, 1 point was given for each questionnaire (the score equivalent to UDI-6 score 1 is 0 point, and that equivalent to UDI-6 score 2 or 3 is 1 point), and the scores of the individual patients as well as the total scores of the patients with and without BOO were presented.
The site and stage of the POP were decided and categorized using the pelvic organ prolapse quantification (POP-Q) system [13]. Statistical analysis was performed using two sample t-tests, the Fisher's exact test, and univariate and multivariate logistic regression analysis, with PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA). A P-value of <0.05 was considered statistically significant.
Results
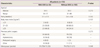
The mean age of the patients with BOO was 54.5 years, and that of the patients without BOO was 58.3 years. The comparison of the two groups (with and without BOO) revealed statistical significance in the presence of menopause. This could be initially associated with the effect of aging, but there was no significant difference in age (Table 1). There were no significant differences either in parity, BMI, history of pelvic surgery, and preoperative and postoperative urinary symptoms, including frequency, urgency, stress incontinence, urgency incontinence, dysuria, and urinary retention. Based on the UDI-6 form, where 1 point was given to each questionnaire, two groups were formed: one with scores of 3 or more and the other with scores of less than 3. Also, there was no significant difference between the UDI-6 total scores of the patients with BOO and those without BOO (Table 2).
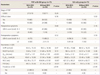
In the POP-with-SUI group, the mean Qmax of the 25 patients with BOO was lower than that of the 50 patients without BOO (10.0 vs. 25.4 mL/sec, P < 0.001). The patients with BOO had a higher mean PdetQmax (49.6 vs. 21.5 cmH2O, P < 0.001), a lower mean MCC (422.7 vs. 454.0 mL, P = 0.007), and a higher mean PVR (44.3 vs. 21.1 mL, P = 0.021). In the SUI-only group, the mean Qmax was significantly lower in the 25 patients with BOO (9.4 vs. 25.4 mL/sec, P < 0.001), and the mean PdetQmax was significantly higher in the same patients (39.6 vs. 25.4 cmH2O, P = 0.004). The patients who had difficult labor were associated with BOO (P = 0.03), and there were no significant differences either in age, BMI, history of pelvic surgery, menopause, and preoperative UDI-6 score, postoperative UDI-6 score, and prevalence of DO (Table 3).
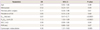
Univariate logistic regression analysis adjusted by group (POP-with-SUI and SUI-only) as a covariate was performed to determine the effects of each component based on the presence and absence of BOO. In the univariate analysis, menopause (P = 0.04; odds ratio [OR], 0.52), MCC (P = 0.04; OR, 0.99), and cystoscopic bladder trabeculation (P = 0.005; OR, 4.36) were associated with BOO. Age, previous pelvic surgery, prevalence of DO, and PVR, however, were not related with BOO (Table 4).
Multivariate logistic regression analysis adjusted by variable, which was significantly different from univariate logistic regression analysis as a covariate, was performed. In the multivariate model, however, no significant association with BOO was found.
Discussion
With the improvement of the quality of life and the gradual increase of the life expectancy of women, the prevalence of women with POP is increasing. As such, the obstetrician-gynecologists are increasingly concerned about POP and other conditions affecting many elderly people, such as UI.
According to population-based studies, 30.4% of the women aged 20 to 59 years in the Swedish population [14] and 40.8% of the postmenopausal women aged 50 to 79 years who were enrolled in the Women's Health Initiative Hormone Replacement Therapy Clinical Trial [1] have some degree of POP. It was reported that the proportion of women with experienced symptomatic POP was about 2.9% (95% CI, 2.1%-3.7%), and that of women with UI was 15.7% (95% CI, 13.2%-18.2%) among the women from 20 to more than 80 years old in a 2008 study in the United States [15].
The important factors affecting POP are history of vaginal delivery, number of vaginal deliveries, elevated intra-abdominal pressure caused by obesity, constipation, chronic coughing arising from a pulmonary disease, and previous pelvic surgery, especially hysterectomy, which may lead to the disturbance of the neural circulation and network [16]. Other factors, such as age and estrogen and vitamin C deficiency, which affect the connective-tissue support, are also known to cause POP [3,17].
The authors' institution reported [4] that the patients with bladder trabeculation were significantly associated with higher mean values of the POP stage compared to the patients without bladder trabeculation (3.13±0.40 and 2.86±0.31, P = 0.023), and that the incidence of bladder trabeculation was significantly higher in the patients suspected of having BOO than those without BOO (80% vs. 46.81%, P = 0.046).
The lack of a standard definition of female BOO, there were trying to define the urodynamic definition of BOO in some previous studies [11,18-21]. In this study, the risk factors for POP of patients with and without BOO, which was defined by the Blaivas-Groutz nomogram [11] (Qmax less than 12 mL/sec and a detrusor pressure at PdetQmax higher than 20 cmH2O), were compared via UDS. There were no significant differences in age, parity, BMI, history of pelvic surgery, home delivery, presence of difficult labor, preoperative and postoperative urinary symptoms, and prevalence of DO between the two groups. Especially, the POP stage had no significant association with BOO (P = 0.24). The outcome may have been derived from the difference in numbers in each stage (of the 75 patients in the POP-with-SUI group, 9, 45, and 21 patients had POP stage II, III, and IV, respectively). Thus, the future study should focus on the correlation between the POP stage and BOO by matching the number of patients in the different POP stages.
The strengths of this study include the fact that it is a serial study of the authors' institution that included more patients than in the previous study. Whereas the previous study suggested possible relationships among bladder trabeculation, the POP stage, and BOO, this study focused on BOO and aimed to compare the factors influencing it as well as to determine its significance in pelvic floor dysfunction patients. Some studies tried to suggest an association between BOO and bladder trabeculation in SUI, but there are no objective evidences of such. This study thus has value in that it held the first trial of the factors related to BOO in SUI. In the multivariate analysis, however, no significant association with BOO was found.
Another strength of this study was its comprehensive evaluation of the factors affecting POP and BOO, for which not only objective evaluation by UDS such as VLPP, MUCP, MCC, prevalence of DO but also subjective factors such as preoperative and postoperative urinary symptoms were utilized, using the UDI-6 form. The Korean version of the UDI-6 form has yet to be validated, but as it is currently being used for the assessment of subjective urinary symptoms in the urogynecology department of many hospitals, it was administered to the patients in this study.
Additionally, all the patients underwent POP surgery and a combination of procedures performed by an experienced surgeon in the authors' institution. Further, as there was only one UDS examiner in this study, inter-observer variation was avoided.
Even though this study had some limitations, a retrospective chart review of 150 patients diagnosed with SUI with and without POP at the authors' institution was conducted. Especially, the UDI-6 form was used in this study to evaluate the preoperative and postoperative urinary symptoms of the patients as self-reported information; as such, recall bias may exist. No significant differences were found, however, in the preoperative and postoperative urinary symptoms, including frequency, urgency, stress incontinence, urgency incontinence, dysuria, and urinary retention, in the comparison of the groups with and without BOO (Table 2).
Another limitation was about the deilemma of definition of BOO. Akikwala et al. [18] reported that the Blaivas-Groutz nomogram overestimated obstruction compared to other criteria. As previously mentioned on other studies, the definition and that following results has been a controversial subject.
In conclusion, objective evidences of the diagnosis of BOO and of the factors related to it in patients with pelvic organ dysfunction were demonstrated in this study, which was a serial study of the authors' institution that aimed to prove the relationship between BOO and cystoscopic bladder trabeculation. Although the results of this study did not have statistical significance, it is believed that a prospective randomized trial targeting more pelvic floor dysfunction patients and comparing to another criteria of BOO is needed to validate the significance of BOO in pelvic floor dysfunction in a preoperative UDS in a future study.


 XML Download
XML Download