

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Perivascular epithelioid cell neoplasms (PEComas) were first described by Bonetti et al. in 1992 [1]. They are rare soft tissue neoplasms with histologically and immunohistochemically distinct perivascular epithelioid cells [2]. They present with clear and acidophilic cytoplasm, perivascular distribution, and immunoreactivity for melanocytic markers such as HMB-45 [3]. They have been described in the liver, lung, pancreas, rectum, and female genital tract [4,5,6]. There have been four reported cases of vaginal PEComas in the literature, two of which were in pediatric patients [6,7,8,9]. Here, we present an extremely rare case of a vaginal PEComa in a 6-year-old girl.
Case report
A 6-year-old girl presented with intermittent vaginal spotting for 6 months. Her urinalysis at a local clinic showed a 2+ positive occult blood test without any other abnormality. The patient was referred to our hospital for further evaluation. She had been diagnosed with pineoblastoma at the age of 2, for which she received three cycles of neoadjuvant chemotherapy and underwent tumor resection. She has been followed up regularly, and her pineoblastoma has been in complete remission without the need for any additional treatment. Her family history was unremarkable. Physical examination and laboratory results were normal except for the 2+ occult blood result on urinalysis. Follicle-stimulating hormone, luteinizing hormone, estradiol and thyroid-stimulating hormone levels were also normal.
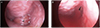
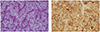
Transabdominal ultrasound showed a normal prepubertal uterus, 2.8 cm in length. Instead of ordering additional imaging studies, we decided to perform a vaginoscopy. Under general anesthesia, she was placed in lithotomy position. Twenty-seven French hysteroscope was gently inserted into her vagina. Using the optical part of the scope, the entire lining of the vagina was inspected. And it revealed a 1.5×1.0-cm benign looking mass arising from the left lateral vaginal wall (Fig. 1A). The mass was completely resected with a wire electrode called cutting loop with clear margins (Fig. 1B). We electrocoagulated the excision site to control the bleeding. Following the surgery, the mass was submitted to the pathology department for review. On histological examination, the tumor showed clear cells with organoid patterns, which is consistent with PEComa (Fig. 2A). Immunohistochemistry of the tumor cells was positive for HMB-45 (Fig. 2B) and TFE3, and negative for cytokeratin, HNF1-B, SOX10, Melan A, and S-100 protein.
One month after the vaginoscopic resection, pelvic magnetic resonance imaging was performed and showed no residual mass without any evidence of lymph node metastasis. Repeat pelvic pelvic magnetic resonance imaging performed 1 year later also showed normal findings.
Discussion
PEComas are very rare tumors that can occur in various sites, and have a non-uniform description. Their natural history and behavior remain poorly understood. They are usually benign but can present with some malignant features [3]. In the majority of reported cases, these tumors behaved in a benign fashion and remained confined to their primary sites of origin [1,2,3,4,5]. However, there have been a few cases of local recurrence and a single reported case of distant metastasis, years after resection of the primary tumor [8,9]. Therefore, they are considered tumors with unknown malignant potential, and there are no proven demographic or morphological criteria predicting aggressiveness or malignant transformation in PEComas [10].
Since these lesions may exhibit an extensive range of biological behavior, there are no well-established treatment guidelines for patients with PEComa [6]. Metastases of PEComa have been successfully managed by resection alone [8]. The role of adjuvant therapy remains unclear. However, if there are some high-risk features such as lymph node metastases, tumor necrosis and a large tumor size, adjuvant chemotherapy can be considered. Patients with PEComa should also be closely monitored for recurrence for long periods of time.
Our case is special because of both the site of the tumor and the age of the patient. Although PEComas have been described in a variety of locations such as the ligamentum teres/falciform ligament, the palate, and the orbit, there have been only a few cases of PEComas arising from the vaginal wall [11,12,13]. In addition, there have only been a few documented cases of PEComas in young children. Among them, our case involves the youngest patient reported to have a tumor arising from the vagina.
The vaginal PEComa in our case was treated with surgery alone because of its small size and benign appearance. Regular follow-up was recommended to this patient because of the unknown malignant potential and recurrence rate. So far no evidence of recurrence has been detected, and we believe that this is due to the early surgical intervention with complete resection. This case shows that early detection and treatment of PEComa is important because of its unknown malignant potential. Since the incidence of vaginal PEComas is very rare, and this is only the third reported case in children, additional case studies are warranted to better understanding of this disease.
 XML Download
XML Download