

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Although serous borderline tumors of the ovary are relatively common, similar tumors of the fallopian tube are rare [1]. We report a tenth case in a 25-year-old woman.
Case report
The patient is a 25-year-old woman, gravida 0, who was referred to the gynecology oncology division at Chonnam National University Hospital with lower abdominal pain and abdominal mass. Her gynecologic history was unremarkable. Physical examination was notable for abdominal mass that was near at xiphoid process. Pelvic ultrasound revealed about more than 20 cm cystic mass. Magnetic resonance imaging of the pelvis revealed about 23×21×9 cm sized serous borderline cystic tumor in the right ovary and 2.2 cm corpus luteum of the left ovary. There was no remarkable findings in the uterus and no abnormal pelvic lymphadenopathy. The tumor marker profile was as follows: CA-125 38.2 U/mL (0-35). Another tumor markers and the result of hematological analyses were within their normal ranges.
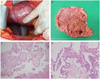
Exploration of the abdominopelvic cavity revealed about 23 cm sized brownish fluid contained cyst located within the right fallopian tube. Its surface was clear and on cut section, it had multiple papillary growing in inner surface (Fig. 1). The left ovary had about 1 cm sized whitish nodule. A right salpingectomy, left ovary wedge biopsy, appendectomy and cytology were performed. A frozen section of the right fallopian tube revealed a serous borderline tumor. And a frozen section of the left ovary revealed a fibroma. Exploration of the right ovary and left tube was unremarkable, and, in view of patient's age and desire for future fertility, no further surgical procedure was undertaken. Histologically, right tubal mass was serous borderline tumor and appendix uninvolved by tumor cells and cytology of peritoneal washing fluid was negative for malignant cells. Tumor had cystic change and papillary nodules. On microscopic examination the papillae were covered by serous type of epithelium (Fig. 1C), displaying stratification and budding with focal nuclear atypia (Fig. 1D). There was no invasion of the supportive stroma of the papillae or into the fallopian tube wall. Micropapillary pattern of the tumor was absent and there was no papillary tubal hyperplasia in the fallopian tube. In general, the histology of the tumor was similar to that of an ovarian borderline serous tumor. Pathologic diagnosis was serous borderline tumor of the right fallopian tube. Close follow-up was recommended and currently, the patient's postoperative recovery was uneventful.
Discussion
To the best of our knowledge, this case is Korea's first report and only ten cases of serous borderline tumor of the fallopian tube have been previously reported in the literature. These cases and current case are summarized in Table 1 [1,2,3,4,5,6,7,8,9]. Age of the patients ranged from 3 to 43 years and the average age was 28.8 years old. The tumors were measuring from 1.7 to 23 cm. Symptoms were non-specific, three tumors were found incidentally [3,4,6], six were presented with abdominal pain [1,2,5,7,8,9]. Most of the patients underwent a conservative surgery as a salpingectomy or a salpingo-oophorectomy [1,2,3,4,5,6,7,8]. In one case, she had a total abdominal hysterectomy and unilateral oophorectomy with partial salpingectromy. Final pathology revealed a serous borderline tumor of the fallopian tube. Thus, she underwent reoperation for complete the staging procedure [1]. In one case, initially a salpingo-oophorectomy was performed. But perioperative diagnosis was serous borderline tumor of the fallopian tube, which led to hysterectomy and a contralateral salpingo-oophorectomy accompanied by an infracolic omentectomy and peritonectomy [9].
In contrast to ovarian tumors, fallopian tube cancers are among the rarest neoplasms of the female genital tract. Adnexal masses of tubal origin are frequently diagnosed as ovarian. Although preoperative sonographic diagnosis of tubal neoplasia is difficult, gynecologists should consider this diagnosis when an adnexal mass is seen in the presence of normal-appearing ovaries. Haratz-Rubinstein et al. [5] have described, the presence of a cystic mass with low-level echoes and mural papillae in the context of normal-appearing ovaries allowed them to suggest a serous borderline tumor of tubal origin. But in our case, tumor size was too large as occupied full abdomen to discriminate the normal ovary from adnexal mass by ultrasound and magnetic resonance imaging. In large sized tumors, sonographic diagnosis of serous borderline tumor of the fallopian tube is very difficult.
Many cases were reported in the literature about giant tumors originating from the ovary. In our case, the patient had a 23×21×9 cm sized tumor in the fallopian tube, occupying a vast majority of abdominal cavity. To our knowledge, this was the largest tumor among the reported cases as serous borderline tumor of the fallopian tube. Kayaalp et al. [4] in 2000, reported a 13×10×10 cm sized serous borderline tumor of the fallopian tube. In another cases, tumor's size measured less than 10 cm.
In most of the reported cases, including current case, conservative surgical treatment was done and surgical staging was incomplete. In only three cases, complete surgical staging procedure was done and final staging was I according to the FIGO (International Federation of Gynecology and Obstetrics) staging system [1,8,9]. The longest follow-up period was 6 years with no evidence of recurrent disease. Zheng et al. [2] reported that nearly 6 years after initial presentation, the patient was alive with conservative operation no adjuvant therapy. To date, there have been no reported cases of metastatic disease.
It is generally agreed that surgical treatment of serous borderline tumor of the ovary should be conservative in those patients who desire to preserve their fertility potential [5]. But there are too few cases in the literature to determine the optimal treatment of serous borderline tumor of the fallopian tube. Therefore, we urge continued reporting of these cases with long-term follow-up period and develop a standard treatment.

 XML Download
XML Download