

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The criteria of preeclampsia have remained unchanged for the past several years. This includes: a proteinuria reading of ≥30 mg (≥1+on dipstick) in two random urine samples collected at least 4 to 6 hours apart or 24-hour urine protein excretion ≥300 mg/day with onset at >20 weeks of gestational age, a systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg measured twice. All of these findings should normalize within the 6th postpartum week [1].
The 24-hour urine protein excretion measurement has been the gold standard for quantifying urinary protein, but it is an inconvenient and time-consuming test. In comparison, the urinary dipstick test may be a quicker and simpler method but its drawbacks are its inconsistency and poor correlation with 24-hour urine protein excretion level [2], because of its susceptibility to patients' hydration status. In this respect, an alternative method that is as simple and rapid as the dipstick test but with better accuracy in predicting the amount of secreted urinary protein would be valuable.
The measurement of a random urine protein-creatinine (P/C) ratio has been tested as a substitute for the 24-hour urine protein excretion test for quantifying protein excretion in patients with renal diseases, such as diabetic nephropathy, lupus nephritis, and transplanted kidneys, with good correlation between the two methods [3-7]. The method relies on calculating the ratio of spot urine protein excretion to creatinine excretion and can normalize the protein excretion to the glomerular filtration rate. Therefore, a random urine P/C ratio is not influenced by variations in hydration status [8]. However, because of the variety of the cutoff values among past studies [9-11], there is no uniform standard so the clinical usefulness of this test is still controversial.
The aim of the present study was to evaluate the ability of the random urine P/C ratio to predict significant proteinuria, as well as to introduce a diagnostic test for preeclampsia that would avoid the inconvenience and time consumption of 24-hour urine protein collection.
Materials and Methods
1. Patients
We enrolled 140 pregnant women who were admitted to Yonsei University Severance Hospital Obstetrics Department with a suspicion of preeclampsia between January 2006 and June 2011. Women with symptoms of preeclampsia and more than one clinical finding, such as hypertension, edema accompanied by rapid weight gain with or without headache, and new-onset proteinuria on a urinary dipstick test, were included. The only exclusion criterion was a concurrent preexisting renal disease such as immunoglobulin (Ig) A nephropathy.
2. Laboratory tests
Firstly, urine was collected via catheterization for the random urine P/C ratio and the urinary dipstick test. Then, a 24-hour urine was collected via a clean catch. Random urine P/C ratio was determined by a Hitachi 7180 Autoanalyzer (Hitachi, Tokyo, Japan).
3. Statistical analyses
Statistical analysis was performed with the SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) and SAS ver. 9.2 (SAS Inc., Cary, NC, USA).
We defined significant proteinuria as 24-hour urine protein excretion ≥300 mg/24 hr. If urine protein excretion was ≥5,000 mg/24 hr, this was considered severe proteinuria, per the guidelines of the International Society for the Study of Hypertension in Pregnancy and the American College of Obstetrics and Gynecology [12,13].
The 24-hour urine protein excretion results were used as a gold standard in determining the cutoff points for the significant and severe proteinuria. Sensitivity, specificity, and positive and negative predictive values of random urine P/C ratio were also calculated against this standard. The correlation between random urine P/C ratio and 24-hour urine protein excretion level was analyzed by regression. Receiver operator characteristic (ROC) curves were evaluated to determine the optimal random urine P/C ratio cutoff value that maximized sensitivity and specificity in the detection of significant and severe proteinuria with 24-hour urine protein excretion.
Results
1. Study population
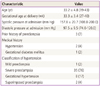
A total of 140 pregnant women were admitted for the evaluation and management of preeclampsia. Among them, 79 were assigned to random urine P/C ratio or 24-hour urine protein excretion. Of these, 71 (89%) were diagnosed with preeclampsia. In 33 of the 79 (42%), either indicated or spontaneous delivery occurred prior to the completion of a 24-hour urine collection; these patients were excluded from the analysis (Table 1). Both the 24-hour urine and random urine samples were available in 46 (58%) patients and their characteristics were as demonstrated in Table 2. The mean maternal and gestational ages were 33.2±4.8 years and 33.3±3.4 weeks, respectively. The mean systolic and diastolic blood pressure was 157.8±20.7 mm Hg and 97.5±9.5 mm Hg, respectively. None of the patients had a history of chronic hypertension or renal disease. Three patients (7%) had a prior history of preeclampsia. Of the 46 patients, 1 (2%) was diagnosed with mild preeclampsia, 35 (76%) with severe preeclampsia, 8 (17%) with gestational hypertension, and 2 (4%), with superimposed preeclampsia, respectively.
Urinary protein excretion was 300 to 5,000 mg per 24 hours in 38 patients (83%) and ≥5,000 mg per 24 hours in 6 patients (13%) (Table 3). Among the enrolled patients, 2 urine samples (4%) measured <300 mg in 24-hours, which did not fulfill for the criteria for proteinuria in preeclamptic pregnancy. The mean collected 24-hour urine volume was 1,448.5±868.9 mL and the mean protein excretion in those sample was 2,713±2,930.2 mg/dL. The mean random urine P/C ratio was 4.2±3.7 (Table 4).
2. Correlation statistic
The correlation coefficient for random urine P/C ratio to 24-hour urine protein excretion was 0.82 (P<0.01), indicating strong agreement between the two tests.
3. ROC curves
The ROC curves for ≥300 mg per 24-hour urine and ≥5,000 mg per 24-hour urine are presented in Fig. 1A, B. The area under the ROC curve of ≥300 mg per 24-hour group was 0.958 (95% confidence interval [CI], 0.903 to 1.000) and for the ≥5,000 mg per 24-hour group was 0.921 (95% CI, 1.074 to 2.002). Analysis of the ROC curve indicated that a random urine P/C ratio of 4.68 was the best cutoff point to detect significant (≥300 mg per 24-hours) proteinuria and to detect severe (≥5,000 mg per 24-hours) proteinuria. The sensitivity, specificity, and positive and negative predictive values were 87.1%, 100%, 100%, and 58.3% for significant preeclampsia and 100%, 85%, 50%, and 100%; for severe preeclampsia. We also compared the area under the ROC curve of the ≥300 mg per 24-hour to that of the urinary dipstick test in Fig. 1C. Each was 0.958 (95% CI, 0.903 to 1.000) and 0.935 (95% CI, 0.883 to 0.899), respectively, demonstrating no significant difference between the two tests. Interestingly, in 4 patients with a negative urine dipstick test but significant proteinuria by 24-hour urine protein excretion, random urine P/C ratio was positive.
Discussion
Mild preeclampsia is defined as a systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg measured twice at least 6 hours apart, with proteinuria of ≥1+ on urinary dipstick test or urine protein ≥300 mg/24 hr. Severe preeclampsia is defined as systolic blood pressure ≥160 mm Hg or diastolic blood pressure ≥110 mm Hg with urine protein ≥5,000 mg/24 hr, sudden oliguria of <500 mL/day, central nervous system manifestations such as headache, visual disturbance, pulmonary edema or cyanosis, epigastric pain, HELLP syndrome, thrombocytopenia, and fetal intrauterine growth restriction [14]. Of these, measuring proteinuria is mandatory for the diagnosis and evaluation of the severity of the preeclampsia. Some studies have found that maternal and perinatal morbidity and mortality increased with the amount of proteinuria [15].
Several methods are available for measuring proteinuria but 24-hour urine protein excretion has long been regarded as the gold standard. However, this test has some disadvantages such as inconvenience for patients, inaccuracy due to incomplete collection, cost, and delay of diagnosis and management, which makes its wide use difficult for clinicians. For this reason, many investigators have explored simpler and more convenient diagnostic methods to quantify proteinuria. One of the most commonly used is the urinary dipstick test because of its simplicity and low cost. Nevertheless, this method has high false positive and false negative result rates associated with fluctuations throughout the day due to water intake, exercise, diet, posture, or improperly trained laboratory staff [16-18]. The urinary dipstick test values of 3+ to 4+ are also not valid for diagnosis of severe preeclampsia because of their very low positive predictive value, which can be as low as 36% [2]. For this reason, a more rapid and accurate diagnostic test that is capable of predicting 24-hour urine protein excretion would be valuable. Here, we propose the use of random urine P/C ratio to facilitate prompt decision making by clinicians [19,20].
Our study compared the diagnostic benefits of random urine P/C ratio to the 24-hour urine protein excretion, the gold standard. From all the enrolled patients, 2 24-hour urine samples (4%) showed protein levels <300 mg, although the values were ≥1+ on the urinary dipstick test. This discrepancy probably occurred due to improper 24-hour urine collection. In fact, previous studies have demonstrated inadequate 24-hour urine collection volume in up to 37% of study samples [3].
The present study demonstrates the value of using the random urine P/C ratio to predict 24-hour urine protein excretion. As shown, a strong correlation was found between the two tests correlation coefficient, 0.82; P<0.01). We also found the optimal cutoff points by analyzing ROC curves for significant (≥300 mg per 24-hours) proteinuria and severe (≥5,000 mg per 24-hours) proteinuria. Also, the cutoff points of 0.63 and 4.68 were found to provide optimal sensitivity and specificity for the detection of significant and severe proteinuria, respectively. This indicates that when a random urine P/C ratio is less than 4.68, it is highly likely that the 24-hour urine protein excretion is less than 5,000 mg (criteria for severe preeclampsia) whereas if random urine P/C ratio is over 0.63, 24-hour urine protein excretion is always over 300 mg. Our results showed no statistically significant correlation between results of random urine P/C ratios and the urinary dipstick tests. However, in the case of 4 patients whose 24-hour urine protein results were more than 300 mg, the urinary dipstick test results were negative, which emphasizes the limitations of the urinary dipstick test method. Meanwhile, in these same patients, the random urine P/C ratios were higher than 0.63, which indicates that it could appropriately diagnose preeclampsia. Therefore, the random urine P/C ratio value could become an effective alternative for making a diagnosis of preeclampsia and can overcome the false negative results of the urinary dipstick test. There are several studies that compare the utility between random urine P/C ratios and the urinary dipstick tests in nephrology units as well as in obstetrics. Gai et al. [21] proposed that the random urine P/C ratio could replace the urinary dipstick test, as they found that the highest regression coefficient was between 24-hour urine protein and random urine P/C ratio (r=0.72), and the lowest between random urine P/C ratio and the urinary dipstick test (r=0.72) in patients with renal disease. They also revealed that the urinary dipstick test failed to detect a pathological proteinuria in 31.6% of their study population while random urine P/C ratio failed to detect in only 5.4%. Meanwhile, in their study with preeclamptic pregnancy, Eigbefoh et al. [22] showed that a random urine P/C ratio had the highest sensitivity, 92%, while the urinary dipstick test had a sensitivity of 81%. Their results also showed that the urinary dipstick test had the highest false negative rate (19%), while that of the random urine P/C ratio was 8%. Furthermore, the specificity for random urine P/C ratio was 86%, while that for the urinary dipstick test was 47%. Also in their study, the false positive rate was highest with the urinary dipstick test (53%), and only 14% for random urine P/C ratios.
Several studies have already established the usefulness of the random urine P/C ratio, including some that have presented evidence of good correlation with acceptable sensitivity in predicting significant proteinuria based on urine collected at different time periods [23-25]. Furthermore, some reports indicate maternal age, gestational age, parity and maternal body size are not confounding factors with regard to random urine P/C ratio [26]. However, some prior studies that evaluated the accuracy of random urine P/C ratio in predicting 24-hour urine protein excretion in preeclampsia reveal some conflicting results for determining an optimal cutoff point for significant proteinuria. This is because of the study-to-study variability in laboratory methods for measuring proteinuria, which precludes valid comparison among the studies. Some reports indicate appropriate cutoff points ranging from 0.15 to 0.5 and sensitivities and specificities from 77.5% to 89.7% and from 72.6% to 80%, respectively [27].
The strength of our study comes from the fact that the random urine P/C ratio was determined before 24-hour urine collection was completed, thereby reducing the potential for a falsely elevated random urine P/C ratio after completion of 24-hour urine collection because of the progression of preeclampsia. However, our study is limited due to its small sample size. Further studies can overcome this issue incorporating a larger study population that also includes outpatient clinic patients.
Based on the results of our study, we conclude that random urine P/C ratios can predict 24-hour urine protein excretion with a high accuracy. This test could be used as a reasonable alternative to 24-hour urine protein excretion, especially in emergent situations, and, it could also complement the urinary dipstick test in preeclamptic pregnancy.




 XML Download
XML Download