

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Placenta previa is a major concern in obstetrics because of the high risk of massive hemorrhage. The need for a hysterectomy is significantly enhanced in placenta previa with a relative risk of 30% to 40% [1,2]. Treatment of obstetric hemorrhage by embolization of pelvic vessels has been widely used as an alternative to surgical intervention that can avoid hysterectomy [3]. There have been new attempts to apply this tool for bleeding control during Cesarean sections. [4].
This study discusses two cases of intraoperative uterine artery embolization (UAE) without fetal radiation exposure in patients with placenta previa totalis.
Case Reports
1. Case 1
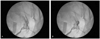
A 40-year-old woman, gravida 0, was admitted to Seoul National University Bundang Hospital in August 2011 for elective Cesarean section and prophylactic intraoperative UAE at 36 weeks and 6 days gestational age. Two thirds of the placenta was located in the posterior wall of the uterus and the remaining placenta was located in the anterior lower segment of the uterus resulting in complete covering of the internal os of cervix. Under spinal anesthesia, a low transverse uterine incision was made and after gently penetrating part of the placenta directly behind the incision site, a live 2,815 g baby was delivered. The upper and lower cut edges and each lateral angle of the uterine incision were clamped using Allis forceps. The torn placental margin was also clamped using Allis forceps. An interventional radiologist, who had been already stood by, stepped into the operation field and then inserted an angiographic catheter into the right femoral artery and approached both uterine arteries using portable fluoroscopy. Insertion of the catheter took five minutes. During that time, the surgeon had observed the uterus carefully for detection of bleeding. Embolization was performed with gelfoam under fluoroscopic guidance for bilateral enlarged tortuous uterine arteries and it took 20 minutes (Fig. 1). After confirming via angiography that there was markedly decreased blood flow, the surgeon removed the placenta. However, bleeding from the implantation site was profuse even though both uterine arteries had been embolized. Bleeding was ultimately controlled by over-sewing the implantation site with 0-monofilament absorbable suture and the rest of the surgery was uneventful. Estimated blood loss for this surgery was 2,500 mL. The patient received five units of packed red blood cells and three units of fresh frozen plasma during the operation. The next day, the patient's hemoglobin was 10.1 g/dL and the sheaths were removed. Routine postoperative care was performed and the patient was discharged from the hospital four days after surgery with no complications.
2. Case 2
A 32-year-old woman, gravida 2, para 0, was admitted to Seoul National University Bundang Hospital at 35 weeks and 5 days gestational age with symptoms of vaginal bleeding in October 2011. Trans-vaginal ultrasonography revealed that the placenta completely covered the internal os. Approximately two thirds of the placenta was located in the posterior wall of the uterus and the remaining portion was located in the anterior lower segment of uterus. When the patient and her husband were counseled about the risk of hysterectomy, they strongly requested preservation of the uterus for future fertility. Therefore, a Cesarean section with prophylactic intraoperative UAE was planned. Under spinal anesthesia, a uterine incision was made transversely at the lower uterine segment. The surgeon could not avoid tearing the placenta before the female newborn weighing 2,465 g was delivered. The torn placental margins and the cut edges of the uterus were clamped by Allis forceps. During the interventional radiologist tried to insert an angiographic catheter into the right femoral artery for four minutes, the surgeon found a diffuse hemorrhage from the torn placental margin and cut edges of the uterus. At this point, the surgeon abandoned the plan of a prophylactic UAE. The surgeon removed the placenta manually and profuse hemorrhage from the placental bed sites developed. Although the implantation site was repeatedly over-sewn with 0-monofilament absorbable suture, bleeding was quite severe, thus a Cesarean hysterectomy was indicated. However, it was decided that intraoperative UAE would be attempted once more before the Cesarean hysterectomy since massive transfusion was successful. The interventional radiologist inserted an angiographic catheter into the right femoral artery and approached both uterine arteries. Embolization with gelfoam was performed under fluoroscopic guidance for bilateral enlarged tortuous uterine arteries (Fig. 2A). Fortunately, blood flow decreased on angiography and bleeding through the vagina decreased. At this point it seemed possible to avoid a hysterectomy. The uterine wall was repaired after an additional intraoperative UAE. Estimated blood loss was 5,000 mL and massive transfusion (9 packs of RBC and 3 packs of FFP) was performed during the operation. Although bleeding decreased markedly after two attempts of intraoperative UAE, the patient was transferred to the angiography room for another attempt at UAE. Embolization of the uterine artery was performed with a coil in the angiography room (Fig. 2B) and then the patient was transferred to the intensive care unit (ICU) for close observation. While in the ICU, the patient received three more packs of RBC and six more packs of FFP as well as cryoprecipitate and platelet. The next day, her hemoglobin level was 10.2 g/dL and vital signs were stable. She was transferred to the general ward for further postoperative care. On the second day after surgery, the patient presented with a fever of 39.1℃ and after a full fever study, her antibiotic regimen was changed. The fever resolved on the fourth day and the patient was discharged from the hospital 10 days after surgery with no other complications.
Discussion
Abnormal placentation, including placenta previa and placenta accrete, is one of the most common causes of postpartum hemorrhage and the most frequent indication for emergent peripartum hysterectomy [5,6]. Recently, UAE has proven to be very effective and is considered the first choice of treatment for patients with postpartum hemorrhage in well-equipped hospitals with skilled radiologists [3]. When applying UAE to patients with postpartum hemorrhage due to placenta previa, the patient must be transported from the operating room to the angiography room. However, only a small portion of patients are hemodynamically stable enough to be transferred for UAE. Intraoperative embolization of pelvic vessels recently has been introduced as an alternative method to reduce expected hemorrhage and ultimately to avoid hysterectomy [7]. All reported cases placed the catheter before starting surgery. Advancement of a catheter under the fluoroscopy is associated with fetal radiation exposure. It has been reported that during this procedure, the fetus is exposed to approximately 3 to 6 rads of radiation in the uterus. A child has an estimated 0.5% risk of developing a childhood cancer following fetal radiation of doses up to 10 rads [8-11]. To resolve these problems, in the cases presented here the catheter was not placed before surgery but an interventional radiologist was prepared for rapid catheterization and embolization, including the presence of portable fluoroscopy equipment (Fig. 3). In case 1, Catheterization itself only took 5 minutes and embolization took 20 minutes. This case is important because UAE was performed successfully before placenta was removed without fetal radiation exposure. However, the total duration of the operation can affect the amount of bleeding and likelihood of infection, which are important issues that must be taken into serious consideration. In case 1, faster closure of the uterus followed by Bakri balloon insertion or postoperative UAE may have been a better choice. Hence, intraoperative UAE should not be performed on all patients with placenta previa. Unfortunately, in case 2, the first attempt at prophylactic intraoperative embolization of the pelvic vessels before placenta removal failed because of profuse bleeding from the torn placental margin and cut edges of uterus before catheterization. Because bleeding from placental bed site was quite severe, the patients could not be transferred to the Angiography room for UAE. Hence, the authors are strongly convinced that the patient in case 2 would have required a hysterectomy if intraoperative UAE had not been performed.
There are many issues which must be addressed for prophylactic intraoperative embolization of pelvic vessels in patients with placenta previa: 1) Indication, which patients with placenta previa need prophylactic intraoperative embolization of the pelvic vessels? 2) Quality of fluoroscopy, a hybrid operation room equipped with high-quality fluoroscopy equipment would be helpful. 3) Method of catheter insertion, preoperative placement of the catheter sheath into the femoral artery under guidance of ultrasound may avoid fetal radiation exposure and reduce the time of angiographic catheterization.
In conclusion, the cases presented here suggest that prophylactic embolization of pelvic vessels under fluoroscopy for patients with placenta previa might help preserve fertility by avoiding a hysterectomy without fetal radiation exposure. However, further studies that establish improved techniques and determine more precise indications for prophylactic embolization are necessary.


 XML Download
XML Download