

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Yolk sac tumor is the second most common malignant germ cell tumor of ovary [1]. This tumor mainly occurs in female children and young women at the median age of 17.6 years. The main clinical symptom of yolk sac tumor is abdominal pain due to the large tumor volume (median size, 14 cm) [1]. The most characteristic pathologic finding of yolk sac tumor is Schiller-Duval body. The glomerular-like process exists in the empty space, and surrounded by tumor cells. The process has blood vessels in its center. This structure is observed in approximately 20% of yolk sac tumor. This structure is not essentially contained for a diagnosis [2]. A a-fetoprotein (AFP) level provides important information on diagnosis, therapeutic effect and recurrence in patients with yolk sac tumor [2]. Yolk sac tumor rapidly grows and metastases via lymphatic and hematogenous route. Most of yolk sac tumors occur in ovary though rarely in extra-ovarian site including mediastinum, sacro-coccygeal region, cervix, vulva, pelvis and retroperitoneum [1-3]. We herein report a case of primary yolk sac tumor of the omentum and literature review.
Case report
A 32-year-old woman was referred to this hospital because of developed low abdominal distension for a month. She got married at the age of 27 years and had no history of pregnancy. She had received diagnostic laparoscopy due to infertility in the past. Menstruation was regular with intervals of 26 days with moderate volume of menstrual fluid and duration.
In physical examination, a palpable mass with abdominal pain and tenderness was found in the right lower quadrant abdomen. CA-125 level was 364 U/mL (normal range, less than 35 U/mL). CA-19-9 level and carcinoembryonic antigen was in the normal range.
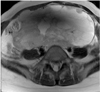
Magnetic resonance imaging (MRI) showed a mass, about 22 ×16 × 8 cm3 in size with ascites and peritoneal seeding nodules (Fig. 1). Findings of intravenous pyelogram, bladder washing cytology, mammography, colonoscopy, and esophago-gastro-duodenoscopy were negative.
Explorative laparotomy was performed and an omental mass, about 23 ×15 ×10 cm3 in size, occupying whole abdomino-pelvic cavity was noted. As frozen biopsy of omentum showed a poorly differentiated tumor though whether it was primary or metastatic was uncertain, total abdominal hysterectomy with bilateral salpingo-oophorectomy, bilateral pelvic lymph nodes dissection, paraaortic lymph nodes sampling, total omentectomy, and appendectomy were performed.
Histopathological result of omental mass showed Schiller-Duval body and both ovaries were not involved (Fig. 2). Right ovary was diagnosed as endometriotic cyst and left ovary was hemorrhagic corpus luteal cyst. AFP level at the postoperative day 7 was high (11,576.67 IU/mL) (normal range, less than 7 IU/mL) though preoperative AFP was not measured.
From the postoperative day 7, 6 cycles of postoperative adjuvant chemotherapy (bleomycin, etoposide, and cisplatin [BEP] regimen) with etoposide 100 mg/m2 and cisplatin 20 mg/m2, each cycle lasting 3 days in combination with 6 cycles of bleomycin 20 U/m2, each cycle lasting 1 day were performed every 3 weeks. In the follow-up after the first chemotherapy, AFP level was found to have decreased to 1,746.15 IU/mL (normal range, less than 7 IU/mL), and in the follow-up positron emission tomography-computed tomography (CT) at 1 month after the sixth chemotherapy, abnormal hypermetabolism suggestive of remnant tumor or metastasis was not observed and AFP level was normal with 2.04 IU/mL (normal range, less than 7 IU/mL). No recurrence was found during the 4-year outpatient follow-up by CT and AFP level.
Discussion
Yolk sac tumor is a rare ovarian tumor and originates typically from reproductive organ. In 10% to 15% of the cases, however, it occurs extra-ovarian region including mediastinum, sacro-coccygeal region, cervix, vulva, pelvis and retroperitoneum, and more rarely in abdomen and retroperitoneum [1,4,5]. Tumors originating from extra-ovarian site can be explained by two major theories. First theory holds that tumors originating from extra-ovarian site occur as a result of aberrant differentiation of somatic cell. By this way, yolk sac tumor can occur in endometrium or stomach. Second theory holds that the tumors originating from extra-ovarian site occur as a result of misplacement of embryo migration in embryogenesis. In the second theory, germ cell is thought to be arrested or misplaced during the migration from cranial cavity, and consequently arrested in the bowel wall or the omentum. The second theory can explain about yolk sac tumor originating from omentum [3,5].
Definite diagnosis of yolk sac tumor can be made by surgical biopsy after evaluation of tumor marker and imaging test. Histological examination with specimen showed the Schiller-Duval body, but Schiller-Duval body is not a essential for a diagnosis. Serum AFP level is a useful marker for diagnosis and treatment including diagnosis of recurrence [6]. In this case, change in postoperative AFP level has important meaning for treatment response. However, in the case of ovarian tumor secreting AFP, it is necessary to histologically distinguish it from other tumors such as hepatocellular carcinoma metastatic to the ovary, hepatoid carcinoma, hepatoid yolk sac tumor, and epithelial ovarian carcinoma. It should be confirmed that no abnormal finding in the liver is shown by re-reviewing the results of imaging test. Hepatoid yolk sac tumor originating from germ cells has been reported to often occur in children and young women. Meanwhile, hepatoid carcinoma has the same histologic findings, but mainly occurs in menopausal women. Hepatoid carcinoma is speculated to originate from the epithelial cells of the ovary. As it requires proactive treatments due to poor prognosis, it is necessary to distinguish it from other ovarian tumors [7].
For the treatment of yolk sac tumor, surgical treatments, combined chemothrapy, and radiotherapy are used. As yolk sac tumor is unilateral, surgical treatment is performed unilateral salpingo-oophorectomy. If metastasis or progression is observed after histological diagnosis confirmed, adnexectomy with debulking operation is conducted [7]. In this case, poorly differentiated tumor was observed in the patient who was young and nulliparous in a frozen biopsy after explorative laparotomy though whether it was primary or metastatic was uncertain. Thus, debulking operation including total abdominal hysterectomy with bilateral salpingo-oophorectomy was conducted instead of fertility-sparing surgery.
Radiotherapy is ineffective, but postoperative combination chemotherapy is very effective in the treatment of yolk sac tumor. Currently, for germ cell tumor, BEP regimen is very effective in patients with initially completely resected tumor. Postoperative adjuvant chemotherapy (BEP regimen) with etoposide 100 mg/m2 and cisplatin 20 mg/m2, each cycle lasting 5 days in combination with 3 to 4 cycles of bleomycin 30 U every weeks is performed in to 3 to 4 cycle every 3 weeks and at each cycle, serum AFP level is measured [8].
We herein report a case wherein surgical treatment combined with combination chemotherapy was performed on a patient diagnosed with a rare yolk sac tumor that originated from omentum and 4-year outpatient follow-up thereafter showed that the treatment was successful.

 XML Download
XML Download