

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Nuchal translucency (NT) measurement is the most powerful screening tool for Down syndrome and congenital malformations, especially cardiac anomaly [1-11]. The Fetal Medicine Foundation (FMF) established the strict guideline for NT measurement. The guideline is used worldwide and requires a certification and annual re-audit for NT measurement. However, to stick to the guideline seems time-consuming and superfluous in some pregnant women whose NT is definitely thin at a glance. We undertook this study to simplify the NT measurement and to investigate whether the simplified protocol is effective in low risk population even if we skip the suggested NT measurement according to the established guideline.
Materials and methods
1. Study population
A prospective study was conducted. Transabdominal ultrasound examination was performed as a part of routine prenatal checks at 11+0 to 13+6 weeks of gestation and the fetal crown-rump length was 45 to 84 mm. The gestational age was basically calculated from the first day of the last menstrual period and was confirmed by crown-rump length (CRL) measurement [12]. If there was some discrepancy of more than 7 days between gestational ages by menstrual calculation and by ultrasound estimation, the latter was used. In cases of multiple pregnancies, the same cut-off value was applied as that of singleton pregnancy [3,13]. All measurements were obtained by one skilled examiner (S.M.K.) with one ultrasound unit, Accuvix XQ (Medison, Seoul, Korea).
The Institutional Review Board of our institution (Seoul National University Hospital, Seoul, Korea) has approved the collection and utilization of clinical and sonographic data for the research purposes.
2. Measurements of 1MV and 2MV
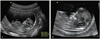
First, CRL was measured in the ordinary view that was mid-sagittal section of fetus in neutral position, and NT was measured at the same frozen screen (first measured value, 1MV) (Fig. 1A). Then, NT was measured three times again according to the FMF guideline (second measured value, 2MV) (Fig. 1B) and out of three measurements, the maximal value was selected. The measurement of 2MV should be met the following criteria [14]; 1) mid-sagittal section of the fetus with neutral position; 2) magnification so that only fetal head and upper thorax included in the image; 3) maximal thickness of the subcutaneous translucency between the skin and the soft tissue overlying the cervical spine; 4) distinction between fetal skin and amnion; 5) the crossbar of the caliper on the white line of the border and not in the nuchal fluid.
We use the standard values of the NT with CRL distribution in Korean population [15].
3. Statistical analysis
Differences between the values of 1MV and 2MV were tested by means of Wilcoxon signed ranks test and associations were described by Spearman's correlation coefficient. Receiver operator characteristic (ROC) curve was used to select the cut-off value of the 1MV that needs to be measured according to the FMF criteria for detection of the 95th percentile or more 2MV. A probability value of <0.05 was considered statistically significant.
Results
Three hundred fifteen fetuses were enrolled. Sixty-seven twin fetuses and seven triplet fetuses were included. In seven patients, NT was so thin that cursors could not be situated at their exact points in the 1MV, and their 2MV values were also very thin, under the 1.0 mm.
There was a good correlation between the 1MV and the 2MV (r = 0.83 by spearman's rho, P<0.001). There was no statistically significant difference between the 1MV and the 2MV by Wilcoxon signed ranks test. All of the NT values over the 95th percentile in the 2MV also belonged to over the 95th percentile in the 1MV.
ROC curve was conducted to examine the relationship between the 1MV and over the 95th percentile 2MV (area under curve, 0.98; P<0.001) (Fig. 2). NT value of 2 mm in the 1MV could be used as a cut-off to obtain the 95th percentile or more 2MV (sensitivity of 100%, specificity of 80.5%, positive predictive value 22.7%, negative predictive value 100%). The proportion of the 1MV ≥2 mm was only 23.8% of all cases, in other words, we had only to measure the 2MV in 23.8% patients. Every 95th percentile or more 2MV could be detected with this simplified protocol. There was no missed case with abnormal NT.
Discussion
In this study, with simplified protocol of NT measurement, we tried to identify low risk women who did not have to undergo the NT measurement by the stringent existing guideline. We have high regard for the established guideline of NT measurement by the FMF, but there was some doubt whether the guideline had to be applied to all pregnant women including low risk population with very thin NT at a glance. We would like to suggest a protocol that identifies low risk women who do not have to measure their fetal NT according to the established guideline and can simplify NT measurement eventually. NT measurement is not diagnostic of any specific disorder with its absolute value, rather, it is just screening process identifies pregnant women who have sufficient risks for Down syndrome or cardiac anomalies to warrant genetic counseling and additional diagnostic tests, such as chorionic villous sampling, amniocentesis, or fetal echocardiography [16]. Our suggestion could be very useful considering the purpose of NT measurement is just to select cases with over the 95th percentile NT values for their CRL.
There is a similar screening test like our simplified protocol in obstetrical field. A 50-g oral glucose tolerance test (OGTT) is a similar example like a simplified protocol. A woman does not have to undergo a cumbersome 100-g OGTT for confirmed diagnosis if her glucose level is under the cut-off in a simple 50-g OGTT. On the basis of our data, 23.8% of pregnant women showed NT measurement ≥2.0 mm at 1MV and almost 3/4 pregnant women can circumvent original NT measurement. It results in decreasing time of examination and medical cost.
The exact value of NT cannot be obtained in some women by our simplified protocol because women whose fetuses have thin NT below 2 mm at the 1MV may skip the measurement according to the established guideline. This may be inappropriate in the combined first trimester screening tests that analyze the results out of maternal serum markers and NT values, both. However, in the centers where the combined first trimester screening tests are not available, our protocol can be useful for saving time and effort in NT measurement. Actually, there are many centers where only NT measurement is used as the first trimester screening test because of various reasons. Especially, the combined first trimester screening test is not covered by national health insurance in Korea.
Considering the role of NT measurement as a screening tool, false positive results can be accepted more generously than false negative results. Our protocol is safe method in this sense. The differences between simplified protocol and the established guideline are proper magnification and identification of fetal skin from amniotic membrane. Neutral position and mid-sagittal section of fetus are also required in our simplified protocol to obtain an exact CRL. Generally, measurement values decrease with increasing image size [17-19]. Therefore, the second MV, in other words, exact NT value measured by the established guideline will have possibility to be somewhat smaller than the 1MV. There were several cases with the larger 2MV than the 1MV in our study. However, most of them had very thin NT measurements. It may be caused by incorrect placement of caliper in the 1MV because the NT is too thin to place the caliper on the exact position without magnification. And if fetal skin is confused with amniotic membrane in the 1MV, the 2MV that measured properly by the established guideline will be further smaller than the 1MV. Therefore, there is little risk missing the abnormal NT values by our simplified protocol. NT measurement of this study was conducted by one skilled examiner. CRL should be measured in the midsagittal plane and it is not always easy to a novice at obstetric ultrasonography. To apply simplified NT measurement, one should be cautious of taking a correct midsagittal plane of CRL.
In conclusion, we suggest a simplified protocol that if the NT is less than 2 mm at ordinary CRL view, the formal measurement according to the established guideline may be skipped. It can be effective for saving time and effort for NT measurements especially in some clinical settings such as multiple pregnancies or where the combined first trimester screening test can't be used.

 XML Download
XML Download