

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Ovarian cancer is the second most common gynecological cancer in Western countries as well as the leading cause of gynecological cancer-related death, with an incidence estimated at 8.8 per 100,000 women-years in USA [1-4]. In Korea, ovarian cancer is also the second most common gynecological cancer, with an incidence of 8.0 per 100,000 women-years in 2010 [4,5]. Though ovarian cancer can be curable in early-diagnosed cases where the disease is limited to the ovary, however most patients are diagnosed when at more advanced stages (International Federation of Obstetrics and Gynecology [FIGO] stage III-IV) [6].
Among gynecologic cancers, the incidence of cervical cancer has been decreasing in Korea [5], which has been attributed to earlier diagnoses secondary to routine pap smears. However, increasing the rate of earlier diagnosis for ovarian cancer has remained difficult due to the relative dearth of associated symptoms and lack of specific serum biomarker.
Currently used as a diagnostic marker for ovarian cancer, cancer antigen 125 (CA-125) is elevated in roughly 80% of patients with ovarian cancer and 30% of patients with other primary cancers with extensive intra-abdominal disease. Accordingly, serum CA-125 levels are not only elevated in ovarian malignancies, but also benign ovarian diseases as well as any other inflammatory conditions of the peritonieum, pleura and pericardium [7-10]. Moreover, as CA-125 levels are elevated in less than half of cases of early stage ovarian cancer [11,12], a new biomarker for ovarian cancer is clearly needed.
First identified in the epithelium of the distal epididymis, human epididymis protein 4 (HE4) was originally believed to represent a protease inhibitor for sperm maturation and contribute to intrinsic immunity. HE4 is also one of 14 homologous genes on chromosome 20q12-13.1 that encodes proteins with a whey acidic protein-type four disulphide core domain [13-15]. Emerging data now suggests that serum levels of HE4 is elevated in ovarian cancer patients, demonstrating similar sensitivity and increased specificity for ovarian cancer when compared with CA-125 [16]. HE4 is also elevated in lung adenocarcinoma, transitional cell, breast, renal and pancreatic carcinomas [17].
In the current study, we analyzed the serum levels of HE4 and CA-125 among patients with ovarian cancer as well as other benign ovarian tumors in order to assess the possible role of serum HE4 levels as an ovarian cancer biomarker.
Materials and methods
1. Study population
In the current case-controlled 1:2 matching study, patients were recruited from Ewha Woman's University Mokdong Hospital in Seoul, Korea between October 2005 and March 2010. Informed consent was obtained in all cases prior to enrollment. The inclusion criteria were: no other diagnosed gynecologic disease except ovarian mass, the ovarian mass had to be the primary diagnosis availability of complete clinical records, informed consent and agreement to have additional testing for new markers, clinical and histological diagnosis with staging and grading of ovarian cancer, according to the current classification and guidelines. And if any cases were not satisfied in criteria, they were excluded.
During the period, 367 women underwent operation, 47 women received a diagnosis of cancer, and 320 women received a diagnosis of benign ovarian tumor. Based on the inclusion criteria, a total of 94 women were enrolled. The 32 cases of ovarian cancer included 16 serous, 5 clear-cell, 5 mucinous, 4 mixed, 2 endometrioid carcinomas. Of 32 ovarian cancer patients, 6 (18.8%) had stage I disease, 4 (12.5%) had stage II disease, 20 (62.5%) had stage III disease and 2 (6.25%) had stage IV disease as per the International Federation of Gynecology and Obstetrics (FIGO) criteria. Histopathology of 62 patients with benign ovarian tumors were as follows: 23 endometriomas (37.1%), 16 mature cystic teratomas (25.8%), 8 mucinous cystadenomas (12.9%), 8 serous cystadenomas (12.9%), 7 other non-specified neoplasms (11.3%). All enrolled patients underwent laparoscopy or laparotomy, and all diagnoses were histopathologically confirmed by pathologic examination at Ewha Womans University Mokdong Hospital.
2. CA-125 and HE4 levels
In all cases, patient sera was obtained on the day prior to the laparotomy/laparoscopy and was stored frozen at -80℃ until analysis.
Serum HE4 levels were measured by HE4 enzyme immunoassay (Fujirebio Diagnostics Inc., Malvern, PA, USA), which were performed as per the manufacturer's instructions. Specifically, the HE4 assay is a solid-phase immunoassay derived from the direct sandwich technique, which uses biotinylated anti-HE4 monoclonal antibody (MAb), streptavidin coated microstrips, and HRP labeled anti-HE4 MAb. To date, no definitive diagnostic thresholds for HE4 have been reported in Korean women, however previous data from other western countries identified 74.2 pM as a cut-off point, as this value corresponded with the upper 95% among healthy individuals from Verona, Italy [18].
Serum CA-125 levels were determined by Modular analytics E170 module (Roche Diagnostics, Mannheim, Germany), an electrochemiluminescence immunoassay derived from the sandwich principle using two monoclonal antibodies, a biotinylated monoclonal CA-125-specific antibody, and a monoclonal CA-125-specific ruthenium complex-labeled antibody. Notably, this assay is able to measure CA-125 levels between 0.600 to 5,000 U/mL, though the manufacturer's suggested cut-off level is 35 U/mL.
3. Statistical analysis
All the data were analyzed using SPSS ver. 21.0 (IBM, Armonk, NY, USA). The median values of the serum HE4 and CA-125 levels were calculated separately for individuals with other benign ovarian tumor and the patients with a diagnosis of ovarian cancer. The relative serum tumor marker levels were compared among the two groups using the Wilcoxon signed-rank test because they did not follow a normal distribution. In all cases, P-values <0.05 were defined as statistically significant.
Receiver operating characteristic (ROC) curves were assessed for both serum values of HE4 and CA-125. Values with the best diagnostic performance as per the ROC curve were identified in order to estimate the area under the curve (AUC).
Results
The clinical characteristics and study groups demographics are presented in Table 1. There were some demographic differences between two groups. The mean age of ovarian cancer group is older than that of benign ovarian tumor group and menopausal patients were more larger in ovarian cancer group.
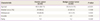
The median serum levels of CA-125 and HE4 were significantly higher among individuals with ovarian cancer when compared with those with other benign ovarian tumors, with the values for each group reaching statistical significance (CA-125, 394.1 U/mL vs. 22.7 U/mL; HE4, 56.7 pM vs. 18.5 pM; P<0.05 in both) (Table 2, Fig. 1).
The patients with benign ovarian tumors were further stratified by known endometriosis as confirmed by a pathologic diagnosis. The median serum CA-125 and HE4 levels were then recalculated for both groups (Table 2) revealing significantly higher serum CA-125 levels in the ovarian endometrioma group when compared with the patients with other benign ovarian tumors (31.95 U/mL vs. 17.9 U/mL, P = 0.03). Conversely, the median serum HE4 levels did not vary significantly between groups (19.0 pM vs. 18.2 pM, P = 0.49). Furthermore, serum CA-125 and HE4 values were compared between patients with ovarian cancer and the ovarian endometrioma subgroup, showing significantly elevated serum levels of both biomarkers among the ovarian cancer group (CA-125, P = 0.004; HE4, P = 0.001).
The ROC curve analysis of the diagnostic performance of patients with ovarian cancer revealed a higher AUC with borderline significance for HE4 when compared with CA-125 (0.93 [95% confidence interval, CI: 0.90-0.97] vs. 0.85 [95% CI, 0.77-0.92]) (Fig. 2, Table 3). Additionally, the AUC for the combination of the two serum markers was 0.89 (95% CI, 0.83-0.95), but a significant difference was not found when comparing HE4 and CA-125 alone.
Using a serum cut-off level of 76.0 pM for HE4 a sensitivity and specificity of 78.1% and 86.8% was observed. Using a serum cut-off level of 37.45 U/mL for serum CA-125, a sensitivity and specificity of 84.4% and 67.4% was observed.
Discussion
CA-125 is the most widely used serum biomarker in ovarian cancer screening, as the utility of CA-125 in determining treatment response or monitoring recurrent disease status has been established [19]. Previous data indicates that at a serum level of 35 U/mL CA-125 has a sensitivity of 73.2% and a specificity of 79.2%, which are comparable to other biomarkers in predicting ovarian malignancy [20]. Nevertheless, CA-125 is not only increased in cases of ovarian cancer but also other benign conditions.
For these reasons, several novel ovarian cancer tumor markers have been assessed for use in screening patients for ovarian cancer, including haptoglobin, osteopontin, HE4, mesothelin (SMRP), B7-H4, prostasin, macrophage colony stimulating factor, vascular endothelial growth factor, several interleukins (IL-6, IL-8), eosinophil-derived neurotoxin, COOH-osteopontin fragments, OVX1, lysophophatidic acid, apolipoprotein A1, and transthyretin [21]. Of these, HE4 has demonstrated high sensitivity and specificity (90% and 77.6%, respectively) in identifying cases of ovarian cancer. In detecting cases of stage I ovarian cancer, HE4 has the highest sensitivity when compared to CA-125, SMRP, CA-72-4, andosteopontin [22].
The results presented here suggest a possible role for serum HE4 as a diagnostic marker for detecting ovarian cancer. Serum HE4 levels were significantly higher in the ovarian cancer group when compared with patients with other benign ovarian tumors (P<0.05), and showed comparable sensitivities in detecting ovarian cancer to CA-125.
Moreover, HE4 demonstrated a significantly lower false positive rate, especially in cases of other benign ovarian diseases such as endometriosis. Several previous studies suggest that serum levels of HE4 are significantly higher in patients with both endometrial and ovarian malignancies, though not ovarian endometriomas or other types of endometriosis. In comparison, serum CA-125 levels were elevated in patients with ovarian cancer, as well as advanced endometriosis with peritoneal or deep lesions, and ovarian endometriomas, though not in the patients with endometrial cancer [23].
As such, we stratified the other benign ovarian tumor group for ovarian endometriomas, as this common benign tumor has been associated with false elevations in serum CA-125 level. In a comparison between groups of patients with ovarian endometrioma versus other benign ovarian tumors, serum CA-125 but not serum HE4 levels were found to be significantly increased in the setting of endometrioma. Accordingly, serum HE4 levels had a lower false positive rate in the data presented here, as in other recent studies.
We also compared AUC for the ROC analysis for CA-125, HE4, and the combination of the two markers. Specifically, HE4 demonstrated a higher AUC than other two groups in distinguishing benign and malignant pelvic masses. In a previous study, risk of ovarian malignancy, showed excellent diagnostic performance for the detection of epithelial ovarian cancer in post-menopausal women, but just the dual marker combination of HE4 and CA-125 did not exhibit any greater accuracy than HE4 alone [18]. In another cohort of Sweden women, HE4 seems like a CA-125 for diagnostic marker for ovarian mass, although the AUC for the HE4 ROC curve is not greater that CA-125. Nonetheless, the sensitivity for HE4 combined with CA-125 was greater than two other serum HE4 and CA-125 group [24]. Given these findings, HE4 may represent a useful diagnostic marker for excluding ovarian cancer in patients with a known pelvic mass.
In the current study, the appropriate cut-off level that yielded a higher sensitivity and specificity was 76.0 pM, a value consistent with data from other studies [18].
Herein, we report early data indicating that serum HE4 levels may represent a new marker for identifying ovarian cancers in Korean women. Until now, many studies for ovarian mass tried to distinguish between ovarian cancer and benign mass in Korean women. Serum CA-125 levels as well as other methods have also been evaluated for ovarian mass screening in Korean women in the past. These previous studies assessed pulsatility index, transvaginal sonographic scoring system and CA-125 preoperatively, and transvaginal Doppler color flow imaging may be useful clinical tools for the differential diagnosis of malignant ovarian tumors [25]. Another study showed that the combination of CA 15-3, Tumor-associated glycoprotein (TAG) 72, and CA-125 may reach an acceptable sensitivity and excellent specificity in differentiating malignant from benign pelvic masses, particularly among patients over 50 years of age. Specifically, these authors collected preoperative serum samples from 78 patients with pelvic masses and measured tumor-associated antigens CA-125, CA-15-3, and TAG 72 by immunoradiometric assay in order to evaluate the efficacy of these markers in differentiating benign and malignant pelvic masses, finding that among patients over 50 years of age the three marker combination was associated with a sensitivity of 79% and a specificity of 100% [26]. Another study of 56 newly-diagnosed epithelial ovarian cancer patients, showed that of five serum biomarkers-leptin, prolactin, osteoponin, insulin-like growth factor-II and CA-125-only the preoperative serum CA-125 level had a significant positive correlation with cancer stage (P<0.01) [27].
With specific regard to the association between HE4 and ovarian cancer in Korean women, the initial study recruited 159 women with adnexal masses, including 78 patients with ovarian cancer [28], as well as 224 healthy controls. In this study, serum HE4 and CA-125 levels were found to be significantly elevated in the ovarian cancer patients when compared with those from patients with benign disease or healthy controls (HE4, 80.0 pM; CA-125, 216.8 U/mL; P<0.0001 in both). But no definitive diagnostic threshold for these tests was ever determined in Korean women. So we need to perform more studies about serum HE4 level in Korean healthy women, then we may determinate the proper definitive diagnostic threshold. A larger case-control study of Korean females was done in 2011. The population of that study comprised 2,182 healthy women, 72 pregnant women, 66 women with ovarian cancers, and 257 women with benign gynecologic disease. The authors suggested an HE4 cut-off level of 33.2 pmol/L for 97% upper reference limits. Using this value as a cutoff point, the sensitivity and specificity for diagnosing ovarian cancer as differentiated from benign gynecologic disease were 90.9% and 94.1%, respectively. The cut-off HE4 level was different from that in our study due to the use of different machines and methods [29].
The primary limitation of the present study is the relatively small size of sample number. As such, no statistical analysis was performed according to the ovarian cancer histological subtype. Furthermore, the serum HE4 and CA-125 levels were also not compared among the healthy controls. A second limitation is that age and menstruation status were not included in the analysis, both of which may have influenced the serum HE4 level. In one prior study, the serum HE4 level increased with increasing age, while serum CA-125 levels were lower in older subjects. However, the upper limits of serum HE4 levels did not vary significantly in the individuals without ovarian cancer regardless of menopausal status [29]. Given these findings, the differences in age between the two groups may have influenced another demographic factor, and a larger scale age-matched case-control study is needed to better characterize this relationship.
In conclusion, serum HE4 likely represents a useful tumor marker for ovarian cancer in Korean women. Assessing serum HE4 levels has the potential to increase the accuracy of ovarian cancer screening and provide better information in differentiating ovarian cancer from other benign ovarian tumors. We did this study as a pilot study and larger, more extended studies are needed to confirm the accuracy of serum HE4 as a tumor marker for the early diagnosis of ovarian cancer in patient with ovarian masses.




 XML Download
XML Download