

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Preeclampsia (PE) is an important cause of maternal morbidity and mortality and is responsible for 6% to 8% of all pregnancies. PE is characterized by high blood pressure and proteinuria that occurs after 20 weeks of gestation. A small-for-gestational age (SGA) infant is defined as an infant birth weight ≤10th percentile [1]; SGA infants have increased fetal morbidity and more severe neonatal complications.
The severity of PE is defined by the amount of protein present in the urine; proteinuria in gravidas with PE is associated with glomerular endotheliosis [2], but the underlying mechanism is poorly understood. The leakage of protein into the urine is a direct result of a disruption of the renal barrier structure in the kidney [3]. The renal barrier has three components, including glomerular endothelium, basement membrane, and podocyte [3]. Karumanchi and Lindheimer [4] counted excreted cells stained for four podocyte markers (podocin, podocalyxin, synaptopodin, and nephrin), noting that all these proteins are in cells excreted by proteinuric pre-eclamptics, but not in the urine of non-proteinuric normotensive gravidas.
Nephrin for SGA development has not yet been established. The pathophysiology for SGA pregnancy was unclear, but known that related to endothelial dysfunction as preeclampsia. Changes in the maternal anti-angiogenic or pro-angiogenic factors such as soluble endoglin or placental growth factor precede the clinical presentation of both preeclampsia and SGA pregnancy. We suggested nephrin was likewise related to SGA development.
Recent studies have demonstrated that defects in nephrin, a protein expressed in the slit diaphragm between podocyte foot processes, causes proteinuria in congenital nephritic syndrome of the finnish type [5,6]. This finding strongly suggests that nephrin plays a critical role in the maintenance of slit diaphragm integrity and renal filtration capacity [7,8].
Although Garovic et al. [2] suggested that podocyturia is a highly sensitive and specific marker for PE, there are no reports demonstrating an association between maternal urinany nephrin and pregnancies complicated by PE and SGA infants before clinical onset.
The objective of this study was to determine the differences in urinary nephrin among controls, and pregnancies complicated by PE and SGA infants. We also determined whether or not maternal urinary concentrations of nephrin are associated with the subsequent development of pregnancies complicated by PE and SGA infants.
Materials and Methods
1. Study population
This was a nested case-control study from an ongoing investigation of PE and SGA infants at Ewha Womans University Mokdong Hospital between 2006 and 2010. The study was approved by the Institutional Review Board of Ewha Womans University and informed consent was obtained from all subjects. Subjects were recruited to the study at the time of the first visit for prenatal care. All subjects, both cases and control subjects, were healthy women without known medical complications. The medical records of subjects were examined regarding pregnancy outcomes by an obstetrician and consisted of uncomplicated control pregnancies (n=50), gravidas with PE (n=33), and gravidas with SGA infants without PE (n=40). PE was defined according to the Working Group criteria [9] as follows: high blood pressure (≥140/90 mm Hg after 20 weeks gestation); and proteinuria (≥300 mg/24 hr).
A SGA infant was defined as an infant birth weight ≤10th percentile, after adjustment for gestational age and gender in an otherwise uncomplicated pregnancy. SGA infants with clinical or pathologic evidence of chronic intrauterine infections or chromosomal abnormalities were excluded from the study. The diagnosis of SGA was determined at the time of delivery. The controls included 50 gravidas, all of whom were monitored in the Department of Obstetrics and Gynecology of our hospital from the first trimester, and who had completed their pregnancies without complications. Exclusion criteria included the following: altered renal function; diabetes or chronic disease; multiple pregnancies; recurrent miscarriages; fetal growth restriction; and intrauterine fetal death. All women with a history of essential hypertension were excluded from this study. Gestational age was defined as the interval between the first day of the last menstrual period and the date of delivery.
2. Urine nephrin concentration
Maternal random, clean-catch urine specimens (50 to 100 mL) were obtained in the first, second, and third trimesters. Urine specimens were collected and frozen at -70℃ immediately after concentration by centrifugation. Urine nephrin concentrations were measured with a commercially available enzyme-linked immunosorbent assay (Exocell Inc., Philadelphia, PA, USA). The assay range is 0.031 to 2.0 ug/mL. The intra- and inter-assay precision for samples in the useful range have coefficients of variation <10% of the mean. Urinary protein and creatinine were determined by standard methods with an automatic analyzer (Hitachi 7180, Hitachi, Tokyo, Japan). The amount of proteinuria was estimated as the ratio of urine protein-to-urine creatinine.
3. Statistical analysis
We used one-way analysis of variance to test the differences of characteristics and outcomes among the study groups and Tukey-Kramer test for multiple comparison. For urine nephrin and urine protein to creatinine ratio, linear mixed model analysis of repeated measures as a continous outcome variables was performed using log transformed data. To examine the differences in mean values of the study groups in each trimesters, Bonferroni method was performed for multiple comparisons. Comparisons of proportions were performed with a chi-square test and Fisher's exact test where appropriate. The Speraman's rho test was used to detect a correlation between two continuous variables. We performed receiver operating characteristic (ROC) curve analysis using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was defined as a probability value <0.05.
Results
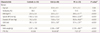
The demographic and clinical characteristics of the study groups are presented in Table 1. Between the controls and SGA group, there were significant differences in gestational age at delivery, birth weight and frequency of preterm births (P<0.05). There were significant differences in body mass index (BMI), systolic and diastolic pressure, gestational age at delivery, birth weight and frequency of preterm births between the controls and PE group (P<0.05). Significant difference between the SGA and PE groups existed with respect to BMI, systolic and diastolic blood pressure, gestational age at delivery and birth weight (P<0.05).
Fig. 1 shows the maternal urinary nephrin and protein-to-creatinine ratio according to gestational age in control group. The more advanced the gestational age was, the higher the levels of urinary nephrin were (P<0.01); however, there was no significant difference in the urine protein-to-creatinine ratio among the three trimesters (P=0.051).
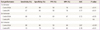
The maternal urinary nephrin concentrations in the SGA and PE groups were significantly higher than controls in the third trimester (P<0.001 and P<0.01, respectively) (Fig. 2). Table 2 shows the log urinary nephrin concentrations in the study groups according to each trimester of pregnancy. Between the controls and SGA group, there were significant differences in the log urinary nephrin concentrations in the first and third trimesters (P<0.05 and P<0.0001, respectively). We also found significant differences in the log urinary nephrin concentrations in the third trimester in controls and the PE group (P<0.01), although there was no significant difference in the first and second trimesters (P>0.05). Although there were no significant differences in the urine protein-to-creatinine ratio between the controls, and SGA and PE groups (P>0.05) (Fig. 2); the log urine protein-to-creatinine ratio was higher in the PE group than controls in the third trimester (P<0.01) (Table 3).
Table 4 and Fig. 3 indicate the test performance of maternal urinary nephrin in predicting SGA infants and PE using ROC curve analysis. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of nephrin in predicting SGA infants were 67%, 89%, 58%, and 76% in the first trimester, 60%, 79%, 69%, and 67% in the second trimester, and 80%, 84%, 58%, and 84% in the third trimester, respectively. In predicting PE, the sensitivity, specificity, PPV, and NPV of nephrin were 67%, 83%, 58%, and 76% in the first trimester and 73%, 79%, 52%, and 82% in the third trimester, respectively. However, there was no significant difference in the urinary nephrin concentrations in the second trimester to predict PE.
Discussion
Our study demonstrates that urinary nephrin is a new marker for predicting PE and SGA infants early in pregnancy. This is the first report regarding the possibility of new markers for identifying pregnancies complicated by PE and SGA infants. Especially, maternal urinary nephrin can be used as an independent marker for SGA infants during the first and third trimesters; however, for the detection of PE, we can use urinary nephrin only in the third trimester.
Recently, Garovic et al. [2] demonstrated that podocyturia (urinary excretion of podocytes) is present in gravidas with PE at the time of delivery and suggested that urinary shedding of podocytes (composed of podocin, podocalyxin, synaptopodin, and nephrin) may contribute to proteinuria in gravidas with PE. This finding from Garovic et al. [2] means that urinary nephrin may indicate nephrin loss from the glomerulus that may lead to a disruption of the glomerular filtration barrier and consequent proteinuria. Garovic et al. [2] also suggested that podocyturia, including nephrin, as a marker of subclinical renal damage, may be detected before overt proteinuria and the full clinical features of PE develops. Based on our results, we showed that nephrin can be a subclinical marker for PE before overt proteinuria. The more interesting finding is that pregnancies with SGA infants without PE have higher urinary nephrin concentrations than controls and urinary nephrin can be used as a subclinical marker during the first and second trimester before the onset of symptoms.
Several studies have provided evidence for altered nephrin expression in gravidas with PE. Zhao et al. [10] successfully cultured shed podocytes in urine specimens from gravidas with severe PE and demonstrated altered expression of slit specific protein nephrin in shed podocytes. Because loss of urinary podocytes is associated with glomerulosclerosis, Sato et al. [11] recommended that monitoring podocyte loss by measuring podocyte products in the urine using mRNA may be clinically useful. For the glomerular expression of nephrin, Garovic et al. [12] first reported that proteinuria in patients with PE is associated with under-expression of nephrin. For the mechanism of nephrin shedding from podocytes in gravidas with PE, Collino et al. [13] suggested that pre-eclamptic sera induces nephrin shedding from podocytes through endothelin-1 release by endothelial glomerular cells, and also identified a potential mechanism of nephrin loss in PE that may lead to endothelial injury with enhanced glomerular permeability. Using a rat model by lipopolysaccharide injection, Beall et al. [14] demonstrated that fetal membranes and placentas of rat express mRNA for nephrin and Neph 1, suggesting a role in the regulation of protein transfer from the fetus to the mother.
We also found that the urine protein-to-creatinine ratio was higher in gravidas with PE than controls in the third trimester and not significantly higher in the first and second trimesters; however, there was no significant difference in the urine protein-to-creatinine ratio in pregnancies with SGA infants during the third trimester because we selected the SGA group as pregnancies without both PE and proteinuria.
Finally, we calculated the test performance of urinary nephrin in predicting SGA and PE using ROC curves. The sensitivity, specificity, PPV, and NPV in predicting SGA in the first and second trimesters were 67%, 89%, 58%, and 76% and 60%, 79%, 69%, and 67%, respectively. In predicting PE, the sensitivity, specificity, PPV, and NPV were 67%, 83%, 58%, and 76% in the first trimester, respectively. Because these test performances, including sensitivity and specificity, of urinary nephrin were >60%, we suggest urinary nephrin is an early subclinical marker, although we need more samples for confirmation.
The main weakness of this study was that we did not match gestational age at delivery and parity among controls, and the SGA infants and PE groups. Another weakness is that we did not determine why urinary nephrin levels in gravidas with PE in the second trimester were more decreased than in the first trimester. Despite these limitations, our study had several strengths. First, it is the first report regarding the possibility of a new marker for pregnancies complicated by PE and SGA infants. Second, we suggest that urinary nephrin measurement by enzyme-linked immunosorbent assay is convenient and easy.
In summary, our results suggest that urinary nephrin can be used as an early marker for prediction of pregnancies complicated by PE and SGA infants, although we need more urinary samples to confirm the association.





 XML Download
XML Download