

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Based on the causal relationship of persistent high-risk human papillomavirus (HPV) infection in cervical carcinogenesis [1], HPV tests have been introduced as part of cervical cancer screening. Since receiving U.S. Food and Drug Administration (FDA) approval, the HPV test has been used to triage equivocal cervical cytology and as a co-test for women aged 30 years and older [2]. The HPV test is more reliable and more sensitive but less specific than routinely performed cervical cytology for detecting cervical intraepithelial neoplasia [3].
Because HPV16 and HPV18 are the most commonly observed genotypes of cervical cancer, a few HPV genotyping tests and Cervista HPV16/18, the first FDA-approved HPV genotyping test, have been validated in clinical trials for assessing persistent HPV infection and detecting cervical precancerous lesions and cancer [4,5]. However, HPV16 and HPV18 are more commonly detected in invasive cancer than in high-grade precancerous lesions, although their rankings appear to be similar [6-8]. In fact, Clifford et al. [9] demonstrated the different squamous cell carcinoma (SCC)/low-grade squamous intraepithelial lesions (LSIL) prevalence ratios of each high-risk HPV genotype, highlighting the importance of individual HPV genotypes for the risk of progression from LSIL to malignancy. Even in in situ cervical cancer, the proportions and rankings of individual high-risk HPV genotypes significantly differed from those of invasive cervical cancer [10]. According to previous Korean studies, aside from HPV16, HPV33, HPV58, and HPV31 were the most prevalent HPV types in cervical cancer, whereas HPV52, HPV58, and HPV51 were commonly detected in precancerous lesions [11-13].
Many data from many countries have been published regarding the type-specific prevalence of high-risk HPV [8,11,13,14], but the results of HPV genotyping surveillance combined with cervical cytology has been rarely reported in the well-organized screening programs for the healthy Korean population [15,16].
Therefore, we conducted a retrospective study to investigate the type-specific risk of high-risk HPV in the development and progression of precancerous or invasive cervical diseases, and to present the foundations for a follow-up guideline for high-risk HPV-positive normal cytology subjects based on the data from routine health care screenings. It is our hope that this information supports the understanding of which HPV types future vaccines should target. As baseline data in this cross-sectional study, we evaluated the type-specific prevalence of high-risk HPV types and their distribution by cervical cytology severity and age.
Materials and Methods
1. Study population
A total of 16,600 women visited Seoul National University Hospital Healthcare System Gangnam Center, Seoul, Korea for a routine health check-up between December 2008 and October 2010. Among the women who were screened, 7,014 consecutive subjects who underwent both a liquid-based cervical cytology (SurePath LBC, Beckton Dickinson, Franklin Lakes, NJ, USA) and an HPV genotyping test by HPV DNA chip (MyHPV Chip, Biomedlab Co., Seoul, Korea) for cervical cancer screening were analyzed in this cross-sectional study. All of the participants were asked to complete systemic questionnaires regarding demographic characteristics, past medical histories, history of surgical diseases, and present medical condition/medication. Information regarding menstruation/pregnancy history, history of contraceptive methods and hormone use, menopausal status, lifestyle characteristics (such as smoking history) and clinical infection regarding gynecologic surgeries, including hysterectomy and/or ovarian surgery, was obtained via direct interview by three expert gynecologists. Based on the responses to the questionnaires and the medical interview, we excluded the following subjects: those with a history of invasive cervical cancer or precancerous lesions, those who had received a hysterectomy and/or bilateral salpingo-oophorectomy and those who had undergone any procedures for treating cervical intraepithelial neoplasm, such as loop excisional electrosurgical procedure, within the previous 5 years. Postmenopausal status was defined as the cessation of menses for at least 1 year or the presence of 40 international units (IU)/L or more of serum follicle-stimulating hormone (FSH). The women were grouped according to age at 10-year intervals from 20 to 60 years. The women aged 60 years or older were grouped in a single comparably sized group.
2. HPV DNA test
DNA isolation was sequentially performed on the remaining suspension of the SurePath Pap test vial. For the HPV genotyping, we used a commercially available HPV DNA chip, which is a PCR-based DNA microarray system. The HPV DNA chip contains 24 type-specific probes for 12 types of high-risk HPV (types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59), four probable high-risk HPV types (types 53, 54, 66, and 68) and eight types of low-risk HPV (types 6, 11, 34, 40, 42, 43, 44, and 70) [17].
Twenty-four type-specific 30-meroligonucleotide probes containing an amine group at the 5'teminus were immobilized onto a chip slide of glass. Each slide had eight chambers, and each chamber was used for a test. Briefly, the target HPV DNA was amplified by polymerase chain reaction (PCR) using the primers (HPV and β-globin) and conditions provided by the Biomedlab Company. The amplified DNA was then labeled with a single dye, indocardocyanine-dUTP (MEM Life Science Products Inc., Boston, MA, USA). The PCR product size of the HPV DNA was 150 base pairs (bp) on the gel electrophoresis. Next, the PCR product was hybridized onto the chip. Hybridization was performed at 43℃ for 90 minutes; the product was then washed with 3×saline-sodium phosphate-ethylenediamine tetra-acetic acid (SSPE) for 5 minutes and 1×SSPE for 5 minutes and dried at room temperature. The hybridized signals were visualized with a DNA chip scanner (Scanarray lite, GSI Lumonics, Ottawa, Ontario, Canada). The samples that showed a positive band of 150 bp on the gel electrophoresis of the HPV-PCR but a negative hybridized signal on the DNA chip scanner were designated as HPV-other samples [18]. None of the negative controls (without DNA) revealed HPV positivity.
Initially, we used an HPV DNA chip that covered 24 genotypes. In December 2009, our institution introduced an HPV DNA chip that identified 19 genotypes covering 11 high-risk HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, and 58) and eight low-risk HPV types (6, 11, 34, 40, 42, 43, 44, and 54); thereafter, HPV59, one of the 12 high-risk HPV genotypes, was omitted from genotyping. High-risk HPV was ultimately defined by Munoz et al. [19] as the presence of one or more of the following 11 HPV types: types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, and 58. Type-specific high-risk HPV prevalence is expressed as the proportion of all high-risk HPV-positive subjects, including all subjects who were positive for either a single infection or a co-infection with HPV genotypes other than the corresponding HPV genotype.
3. Cervical cytology
Independent of the HPV testing result, all of the cytologies on the slides were read according to the routine laboratory protocol and reported a cytological classification based on the Bethesda nomenclature system [20]: squamous cervical carcinoma/adenocarcinoma, high-grade squamous intraepithelial lesions (HSIL), atypical squamous cells, cannot exclude HSIL (ASC-H), atypical glandular cells (AGC), LSIL, atypical squamous cells of undetermined significance (ASCUS) and negative. A panel of cytopathologists was masked to the HPV DNA chip test results. To analyze the trends of individual HR-HPV genotypes distribution, all cervical cytologies were grouped as follows: negative, ASCUS/LSIL, and HSIL or worse. Because of their substantial likelihood of developing cervical cancer [21], 11 subjects with ASC-H were categorized as HSIL or worse; two subjects with AGC were excluded from the study population.
4. Statistical analysis
The baseline characteristics of continuous variables were compared using Student's t-test. For categorical variables, the chi-squared (χ2) test or Fisher's exact test was used. The data were analyzed with SPSS ver. 19.0 (IBM, Armonk, NY, USA), and two-sided P-values <0.05 were considered statistically significant.
Written informed consent was obtained from all participants. This retrospective cross-sectional study was approved by the Institutional Review Board of Seoul National University Hospital (IRB-No. H-1012-095-344).
Results
1. Baseline characteristics
A total of 7,014 women with both cervical cytology and HPV test results were enrolled. The mean age of the participants was 48.2±9.2 years, and 81.5% were aged 40 years or older. The clinical characteristics of the subjects are shown in Table 1. The overall prevalence of abnormal cervical cytologies (ASCUS or worse) was 4.7%, showing a U-shaped trend according to age groups: the highest prevalence was in the youngest group, the lowest was in the 30- to 39-year-old group, and there was a slight increase in the oldest group (13.2%, 2.7%, and 3.9%, respectively) (Fig. 1). Squamous cervical carcinoma in the cervical cytology was noted only in two subjects.
The overall positivity for any HPV and high-risk HPV was 19.7% and 8.4%, respectively. When the HPV prevalence was reexamined with regard to the HPV DNA chip probes, no significant difference in the overall prevalence of high-risk HPV was observed between the two probes of the DNA chip (9.3% for the 24-probe chip and 8.3% for 19-probe chip, P=0.131). In comparison, the overall prevalence of any HPV was significantly higher with the 24-probe chip than with the 19-probe chip (21.9% vs. 18.2%, P<0.001), whereas the prevalence of HPV-other was significantly lower with the 24-probe chip than with the 19-probe chip (33.8% vs. 44.2%, P<0.001; data not shown).
2. Prevalence and distribution of high-risk HPV types according to age groups
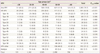
The overall prevalence of any HPV and high-risk HPV declined markedly with age (P for trend<0.001 for each) (Table 2). The youngest group had the highest positivity for high-risk HPV, and the oldest had the lowest positivity, showing an age-dependent decrease (29.0% and 5.5%, respectively; P for trend<0.001). In contrast, the proportion of HPV-other showed a significant age-specific increase (P for trend<0.001). There was no age-specific trend for low-risk HPV prevalence.
We then calculated the proportion of individual high-risk HPV types among high-risk HPV positive-subjects. In total, the most prevalent HPV types were HPV58 (23.9%), HPV16 (21.8%), HPV52 (16.6%), HPV18 (11.7%), HPV33 (9.0%), and HPV35 (9.0%), in order of frequency.
Regarding the age-specific prevalence trend of individual high-risk HPV types, there was a marked decline in the proportion of HPV52 with age, ranging from 21.1% in the youngest group to 11.4% in the oldest group (P for trend=0.014). Among women aged 30 years or older, the proportion of HPV39 also progressively decreased with increasing age (P for trend=0.051, data not shown). The proportion of the other high-risk HPV types, including HPV16, did not vary significantly according to age group. Co-infection with several HPV types was detected in 19.0% (262 out of 1,380) of the HPV-positive women and was markedly prevalent in women aged 30 years or younger, but showed no significant age-specific trend.
3. Prevalence and distribution of high-risk HPV types according to cervical cytology
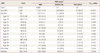
The prevalence of any HPV, high-risk HPV and the proportion of individual high-risk HPV genotypes according to cervical cytology are shown in Table 3. As a whole, the prevalence of any HPV and all high-risk HPV types increased progressively with increasing severity of cervical cytology (P for trend<0.001, respectively). For low-risk HPV, no age-specific trend was observed.
In terms of individual HPV genotypes, only HPV56 showed a strong increase in proportion with cervical cytology severity (P for trend=0.041), ranging from 7.2% of subjects with normal cytology to 11.7% and 12.5% of subjects with ASCUS/LSIL and HSIL or worse. Among women aged 30 years or older, the positivity of HPV52 and HPV56 was marginally related to abnormal cervical cytology (P=0.055 and P=0.058 for each, data not shown). For the other high-risk HPV genotypes, including HPV16 and HPV18, no significant type-specific trends were observed according to the cervical cytology severity.
Co-infection with several HPV types also significantly increased with the severity of cervical cytology (P for trend=0.029). Among the high-risk HPV-positive women who had abnormal cervical cytology (≥ASCUS), 45.4% (54 out of 119) tested positive for more than one HPV type. The positivity of HPV-other significantly increased with the increasing severity of cervical cytology (P for trend=0.026).
Discussion
The principal finding of our study was that the most prevalent HPV types were HPV58, HPV16, HPV52, and HPV18, all of which accounted for 73.9% of the 591 high-risk HPV infections detected. In terms of individual HPV types by cervical cytology and age, there was a significantly increased prevalence of HPV56 with cervical cytology of increasing severity. The prevalence of HPV 52 had a marked age-specific decline but a marginal incease with cervical cytology severity among women aged 30 years or older. Additionally, an age-specific decline in the overall high-risk HPV prevalence was reaffirmed independent of cervical cytology, except for HSIL or worse (Fig. 2).
Among women aged 30 years or younger, the prevalence of any HPV and high-risk HPV reached peak; however, there was no discrete trend in type-specific HPV prevalence by cervical cytology. The overall prevalence of abnormal cervical cytology (ASCUS or worse) also peaked in the youngest age group (Fig. 1). In the youngest group, however, no subjects had severe abnormal cervical cytology (HSIL or worse), whereas all of the subjects with SCC were in the oldest group (data not shown). These findings correspond well to the background of the revised American Society for Colposcopy and Cervical Pathology (ASCCP) guideline [22] and can be supported by the study by Trottier et al. [23] on incident HPV infection and the timing of cervical lesions in young women. They reported that women who did not experience an HPV infection had a very small risk of developing a lesion, but that a transient high-risk HPV infection as short as 3 months was associated with the risk of cervical abnormality, and persistent cervical high-risk HPV infection, specifically with HPV16/18, was a much stronger predictor of cervical lesions.
Of all of the HPV-tested subjects, HPV58 was the most common type in normal or mildly abnormal cervical cytology (ASCUS/LSIL), consistent with other data on type-specific HPV prevalence in either Korean or Asian populations. However, in our study, the prevalence of HPV58 did not have a significant association with the severity of cervical cytology, unlike other studies in which there was the high prevalence of HPV58 in both HSIL and SCC [24,25].
A significant type-specific trend toward cervical cytology severity in our study was observed only for HPV56. Among women aged 30 years or older, the prevalences of HPV52 and HPV56 were marginally associated with abnormal cervical cytology. Despite the small number of subjects with abnormal cervical cytology (including only one HPV56-positive subject who had HSIL or worse), the prevalence of HPV56 was relatively high, specifically in abnormal cervical cytology, compared with the prevalence reported in other studies [13,26]. In the study by Choi et al. [26], HPV56 had a relatively low prevalence, but it was more commonly detected in low-grade cervical intraepithelial neoplasia (CIN) than were HPV16, HPV58, and HPV52. HPV52 has been often noted as one of the prevalent high-risk HPV types in precancerous lesions in the Korean population, followed by HPV16, HPV18, and HPV58 [27,28]. In comparison, the prevalence of HPV16 in our study was considerably low (1.8% of the women overall and 21.8% of the high-risk HPV-positive women), with only a 12.5% prevalence among the 22 subjects who had HSIL or worse. All of these findings are inconsistent with the findings of other studies [24,25,29-30]. Most studies have reported that HPV16 was the most prevalent type [6,10,29,30], reaching an overall prevalence of 3.3% and a range from 1.5% in normal cytology to 45.6% in HSIL+ and 9.7% at age 20 to 29 years to 0.7% at age 50 to 64 years [29].
One possible explanation for our findings' inconsistency with other studies is that the proportion of young women (<30 years old) was very low (only 1.9%) in our study population. The predominance of HPV16 in young women has been already noted across the cervical disease categories [10,31,32]. Some authors have demonstrated that the age at diagnosis of HPV16- and HPV18-related invasive cancers was 5 years earlier than the age of diagnosis for cancers caused by high-risk HPV types other than HPV16/18, suggesting that the age of first cervical cancer screening could be delayed in the HPV-vaccinated population [10].
Another possible explanation is that our study population consists of apparently healthy people who voluntarily seek health check-ups and thus have a substantially low prevalence of abnormal cervical cytology (less than 5%). In a recent population-based study, HPV16 was the most commonly encountered HPV type even in normal cervical cytology, but its prevalence was substantially low among all tested women [33]. It has also been noted that the performance of each of high-risk HPV detection methods differs when applied to the detection of genital HPV DNA, especially in cervical swabs with low grades of dysplasia or normal cells [34]. Presumably, the relatively much lower detection rate of HPV DNA in our study population is related to the lower levels of HPV DNA in these specimens [34,35].
Finally, we assume that individual HPV types have different potentials to develop abnormal cytology from normal uterine cervixes, similar to those involved in the progression from LSIL to SCCA suggested by Clifford et al. [9]. Despite the fact that HPV16 and HPV18 are the most commonly detected high-risk HPV types, the prevalence and distribution of the high-risk HPV types that are prevalent in precancerous lesions differ greatly from those of cervical cancers, depending on the subjects' race and geography [29,36,37]. In addition, it can be also supported by the fact that the efficacy of the HPV vaccine has been attributed to its protection against lesions associated with non-vaccine HPV types, which are shown to be higher against CIN3+ than against CIN2+, thereby indicating the greater contribution of HPV16 and HPV18 to precancerous lesions of increasing severity [38].
Regarding co-infection with several HPV types, the proportion of HPV16 in our study was inconsistent with that reported in other studies. According to ARTISTIC trial data, the proportion of women positive for HPV16 as a single infection increased with increasing severity of cervical cytology, thus suggesting that HPV16 may compete with less virulent types in the progression to neoplasia rather than in normal infective processes [29].
In our study, only 30.9% (103 out of 333) of the subjects who had high-risk HPV-positive ASCUS or LSIL+cytology had available histologic confirmation data. Among the 15 of these 103 subjects who had CIN2 lesions or worse (CIN2+), only 13.3% were positive for HPV16 (95% CI, 1.7% to 40.5%); in all cases, HPV16 was present a as co-infection with other high-risk HPV types. In contrast, the positivity of high-risk HPV types other than HPV16 (i.e., HPV52 and HPV58) was to some extent higher than that of HPV16 (20.0%, 95% CI 4.3% to 48.1% for each). As single infections, the proportions of HPV52 and HPV58 were much higher than that of HPV16 (for HPV52, 13.3%, 95% CI 1.7% to 40.5%; for HPV58, 6.7%, 95% CI 0.17% to 32.0%; for HPV16, 0.0%, 95% CI 0.0% to 21.8%). Considering the prevalence and distribution of HPV52, HPV56 and HPV58 by cervical cytology and age, our study's findings may support the hypothesis that by showing different potentials, high-risk HPV types other than HPV16/18 may play great roles the development of abnormal cervical cytology or precancerous lesions in the normal cervix in the general population. These findings are also consistent with the high-risk HPV types detected in the progression to cervical cancer [24-26,29,38].
Our study has some other limitations. First, because of its cross-sectional design based only on cervical cytology, the attributable type-specific risk of high-risk HPV for cervical precancerous lesions and invasive cancer could not be assessed. However, a further study with follow-up data is being planned with the hope of finding evidence of the role of individual high-risk HPV types in the risk of progression to precancerous lesions and invasive cancer. A recent study by Kjaer et al. [30] reported a good correlation of prevalent high-risk HPV type distributions between subjects with abnormal cervical cytology and those with cervical disease, such as histologically confirmed CIN; based on that study's findings, we can anticipate that individual high-risk HPV types that gradually increase in prevalence with increasing severity of cervical cytology, appear to correspond to the HPV types commonly detected in high-grade CIN.
Second, the prevalence of the individual high-risk HPV types in our study is determined by a mathematical sum of both single infection and co-infection with several HPV types other than the corresponding HPV type; therefore, the totals are often greater than 100%. Still, there are no established methods or analyses for addressing the complexity of co-infections with several HPV types, although some authors have developed mathematical models or HPV type assignment algorithms to estimate the contribution of each high-risk HPV type to the development or progression of precancerous lesions and invasive cancer when several HPV types are detected [39,40].
Finally, our study population consisted of healthy subjects who lived primarily in a metropolis and were interested in their health, as they voluntarily participated in the private screening program. These subject characteristics may have led to the very low prevalence of abnormal cervical cytology and CIN, consequently requiring cautious interpretation of our results.
Despite these potential limitations, our study has several advantages. First, to our knowledge, it presents the largest Korean study population to date that includes a wide age range, and combined cervical cytology and HPV genotyping test using an HPV DNA chip for primary cervical cancer screening [11-13]. Second, our study population consists of apparently healthy people who sought health check-ups, which we hope will help to elucidate the natural history of HPV infection and its relationship with the development of cervical diseases.
In conclusion, our finding is that the prevalence and distribution of specific HPV types by cervical cytology and age in the apparently healthy population differs significantly from the HPV type distribution and prevalence detected in patients with cervical cancer and precancerous lesions. Given important role of HPV in the pathogenesis of cervical cancer, the development of precancerous lesions and the progression to invasive cancer, we can hypothesize that similar to the progression from LSIL to malignancy reported by Clifford et al. [9], high risk-HPV types other than HPV16 might play a role in the progression from a normal cervix to mild cervical diseases [8]. This hypothesis implies that by identifying the specific high-risk HPV types with different carcinogenic potentials, HPV genotyping test shows clinical relevance in cervical cancer screening programs for the follow-up of type-specific persistency and triage for women aged 30 years or older.



 XML Download
XML Download