

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Osteoporosis is a public health issue with high prevalence worldwide. The incidence of the disease in 1990 was 1.66 million people with a projection of 6.26 million cases in 2050.[1] In Brazil, it is estimated that 140,000 subjects will have osteoporosis until 2020.[23] The disease is an economic burden for the Brazilian National Health System, costing United States Dollar 72 million between 2008 and 2010.[4] Therefore, intervention strategies need to be planned and performed to address the risk factors related to osteoporosis. Regarding this issue, evidence shows that childhood and adolescence are crucial periods of bone formation and bone accrual during these phases determines bone health in adulthood.[5] During the peak height velocity (PHV), there are several factors influencing bone mineral density (BMD), such as genetics, hormonal levels, and lifestyle habits.[678]
Physical activity during childhood and adolescence is considered a prevention factor to osteoporosis, given that sports participation promotes BMD accrual and maintenance.[9] Moreover, gains in BMD through sports participation during adolescence can persist throughout life.[1011] Physical activity has different contexts and sports participation is the most frequent among youth.[12] The osteogenic effect of sports participation on bone health occurs in two ways: internal (muscle contractions) and external (impact generated by the practice in the sport).[13] It creates tension in the bone matrix, increasing the concentration of formation markers (osteoblasts) in the tissue and, consequently, modifies the skeleton to support the new activity.[13]
The impact of different sports on bone health, such as soccer, basketball, gymnastics, swimming and tennis, is already described in the literature.[9141516] However, there are still doubts about track and field, a sport composed of different competitions (races, jumps, throws, and combinations).[17] Due to track and field's mechanical impact, theoretically, it can improve BMD by promoting stress of bone matrix and producing essential growth changes of the bone structure.[18] However, previous studies are not in agreement. Bush [19] found a protective effect of running in BMD among girls, as well as Greene et al.[16], which also showed a protective effect of track and field on BMD. On the other hand, Lucas et al.[20] found no association between track and field and bone mass. Moreover, most of the studies did not evaluate the effect of sports participation among boys.
Therefore, this study aimed to compare BMD in different body segments among adolescents engaged and not engaged in track and field, using a pilot sample of the Analysis of Behaviors of Children During Growth (ABCD - Growth Study). Our initial premise states that BMD would be higher among track and field athletes than in non-active adolescents (controls), even after adjustments for potential confounders.
METHODS
The longitudinal research entitled ABCD – Growth Study is an on-going study dedicated to identifying the impact of sports participation on different health aspects of adolescents, including bone health. The present study is part of the ABCD – Growth Study, which is being carried out in Presidente Prudente, São Paulo, Brazil. Data collection and analyzes were performed by members of the Laboratory of Investigation in Exercise (LIVE) in 2017, which is part of the Department of Physical Education of the São Paulo State University (UNESP). The ethics committee of UNESP approved the study (process number 1.677.938/2016). All the parents and responsible for the adolescents signed the consent form, and the coaches responsible for the athletes also signed an authorization form.
1. Population
In the present study, we used a pilot sample of ABCD - Growth Study. Thirty-four adolescents of both sexes composed the sample (22 boys and 12 girls), 17 track and field adolescents and 17 adolescents in the control group (the sample was paired by age [1 athlete by one control]). Control group was recruited from schools located in the metropolitan region of the city, while athletes were recruited from a track and field training center in the city. The inclusion criteria were: (1) 11-18 years-old; (2) parents' consent form signed; (3) if athletes, at least one year of track and field training experience; if control group, at least one year without practicing any sport or exercise. Adolescents in the track and field group practiced three to six times per week, with two hr of duration per session.
2. Anthropometry and somatic maturation
Body weight (kg) was measured using a digital scale (Filizzola PL 150; Filizzola Ltd., São Paulo, Brazil) and height (cm) was measured using a stadiometer with a precision of 0.1 cm. Both measurements were collected using standard protocols. Body mass index (BMI) was estimated using body weight and height. Also, analysis of the sitting height and the length of the legs were performed to calculate the years from PHV, which denotes the time (years) from/to the age at PHV (APHV), an indicator of biological maturation timing.[21] APHV is an important event of the biological maturation process, which can influence body composition and bone variables.
3. Body composition and bone variables
Body composition (body fat [kg], lean mass soft tissue [LST; kg], BMD [g/cm2] and bone mineral content [BMC; g]) of whole body, lower limbs, upper limbs, trunk and column was assessed using a dual energy X-ray absorptiometry (DXA) scanner (Lunar DPX-NT; GE Healthcare, Little Chalfont, Buckinghamshire, UK) with GE Medical System Lunar software (version 4.7). DXA measures were performed in the morning after a light breakfast, and the scanner quality was tested by a trained researcher before each day of measurement, following the manufacturer's recommendations. The participants wore light clothing, without shoes and remained in the supine position on the machine (approximately 15 min).
4. Vitamin D intake
A questionnaire with foods rich in vitamin D commonly observed in Brazilian diet was applied, in which a score of vitamin D intake was generated from the sum of the values.[9]
5. Volume and overload of training
The track and field group reported the number of days per week involved in the sport, as well as the time (min) and intensity (scale of perceived exertion [10]) of each day engaged in practice. The daily overload was calculated by multiplying the intensity by volume.
6. Statistical analysis
Descriptive statistics were used to describe the sample, with values of mean and standard deviation (SD). Student's t-test for independent samples was applied for comparison between groups and analysis of covariance to verify differences in BMD and BMC adjusted by covariates (sex, years from PHV, vitamin D intake and lean soft tissue of body member). Statistical significance was set at P<0.05 and all analyzes were performed using BioEstat version 5.2 (BioEstat, Tefé, Brazil).
RESULTS
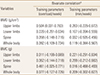
Our sample was composed of 34 adolescents (22 boys) with a mean age of 16.0±1.09 years old. Track and field athletes presented higher anthropometric values (Height and fat mass) with significant differences compared to the control group (P=0.01). On the other hand, there was no significant difference for LST, years from PHV, and APHV between athletes and controls. Regarding bone variables, the athletes showed the highest BMD in lower limbs (total [P=0.003] and segmental [P=0.004 in left leg and P=0.002 in right leg]), and whole body (P=0.025) (Table 1).
Regarding BMD and BMC, considering the effect of confounding variables, there were similar characteristics between the control group and the track and field group. However, years from PHV (P=0.040; effect size eta-squared [ES-r]=0.142) (Table 2) and LST (P=0.01; effect size ES-r=0.487), Table 2 were the factors that most affected bone outcomes and, therefore, presented the highest clinical relevance.
Among girls, BMD and BMC presented similar values comparing control and the athletes in the adjusted analyses. Similarly, LST [ES-r=0.340] and years from PHV [ES-r=0.167] also had high clinical relevance for bone variables (Table 3). Among boys, BMD and BMC did not differ between athletes and controls, although, after adjustment for LST (P=0.01), it showed a high clinical impact on BMD and BMC [ES-r=0.498] (Table 4).
Finally, Table 5 shows the relationship between overload and volume of training with BMD and BMC. The track and field group demonstrated a positive relationship between training load and BMD in upper limbs (r=0.504; 95% confidence interval, 0.031-0.793).
DISCUSSION
This study aimed to compare bone variables of adolescents engaged or not in track and field, as well as to understand the effect of training overload/volume on bone health. Our results showed, in the crude analysis, that athletes presented higher BMD in lower limbs and whole body, and higher BMC in lower limbs and right arm when compared to the control group. However, when considering the effect of sex, maturation, vitamin D intake and LST, the groups presented similar results. LST was the variable with the greatest effect on the outcomes for both sexes, and training overload was positively related to BMD in upper limbs.
Track and field is a sport that requires intense activity in the lower limbs during its practice, and it is incredibly effective for muscle mass gain. Therefore, higher values of BMD in lower limbs is easily justified by the literature and corroborated by other studies. As proposed by Magkos et al.[22], practice of track and field during adolescence may lead to better bone health in adulthood.
However, the adjusted models showed no effect of track and field practice on bone outcomes, given that fat-free mass (most elevated effect in BMD and BMC) had a bigger effect on these variables. The peak of muscle growth precedes peak of BMD.[23] Therefore, muscle mass increases before bone. However, in the context of sports, one of the justifications for the effect of muscle mass on bone health is related to the mechanical overload of muscle contraction in the bone tissue, favoring greater tissue adaptation. [24] Track and field is a sport that involves several competitions and training methods almost always use muscular strength (snatch, and clean and jerk), working the whole body.[25] According to a meta-analysis conducted by Behringer et al.[26], strength training, jumps, and running have positive effects on bone health, showing gains of BMD and BMC. Thus, LST should be a possible mediator factor of the association between track and field practice and BMD/BMC. Although we did not adopt the exact mediation process in our study due to sample size, future research should investigate this topic in a larger population.
Somatic maturation was also identified as a possible mediator of the association between sports practice, BMD, and BMC. Biological maturation affects all human tissues,[8] including bone. The peak of BMD and BMC occurs around one year after APHV [27] because bone mineral accrual happens following longitudinal growth. On average, our sample is inside the range mentioned above. Thus, it is natural that adolescents with advanced maturation presented greater BMD.[8] Moreover, it is also expected that sports participation has a higher effect in adolescents with delayed maturation (yet passing through maturation process).[510] However, maturation should also be tested in future research with greater sample size.
Studies have emphasized that sports participation has provided gains in BMD and BMC.[528] Although track and field involve modalities of throwing, requiring a little more of the upper limbs, significant differences were found only in BMC of the right arm. However, when adjusted for confounding factors, the difference disappears. This result can be explained by the more significant effect of LST on BMC gain, and the difference only in the right arm points out to a possible degree of dominance among the limbs. In contrast to our findings, Whittington et al.[25] analyzed BMD and BMC of college students compared to a control group and other sports, and found higher BMD and BMC in upper limbs. Thus, in the present study, the positive effect of track and field on lower limbs BMD seems to happen due to the impact exerted by LST.
Additionally, when analyzing the relationship between training overload, BMD, and BMC, we found a positive correlation with upper limbs BMD, highlighting the greater effect of practice on BMD.[29] Even among adolescents, an increase in training volume was sufficient to improve trabecular and cortical densities.[30] However, this association can also be associated with an increase in muscle mass caused by the continued sports participation.
One of the limitations of the present study is the vast possibilities of engagement in track and field, which involves different events, such as jumps, throws, speed races, and endurance races. The characteristics of each of these events may affect bone health differently, and new studies should be conducted comparing different track and field athletes. Although we used a questionnaire to assess vitamin D, which is an accessible and non-invasive method, it was not possible to quantify the sun exposure (mostly responsible for the production of Vitamin D). Possible mediators also were not investigated, such as serum levels of hormones and inflammatory cytokines, variables that can influence bone formation. Finally, a bigger sample size is needed for more complex analyses.
In conclusion, track and field participation in adolescence appears to influence BMD and BMC in lower limbs, and fat-free mass seems to mediate this effect. Also, higher training loads were found to be positive for bone health in upper limbs.




 XML Download
XML Download