

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bisphosphonate is effective for the treatment of osteoporosis, and prevention of osteoporotic fractures. Practically, several types of bisphosphonates have been available in prevention of osteoporotic fractures.
Although the efficacy of several bisphosphonates in elderly patients have been previously presented in prospective randomized clinical trials (RCTs),[1234] the optimal choice of bisphosphonate for osteoporotic patients remains controversial. Although RCT are believed to provide the highest level of evidence regarding the merits of procedures, RCT does not provide a decision guide which bisphosphonate should be choose. Moreover, there was no RCT that with head-to-head comparison of bisphosphonate.
On the other hands, decision analysis is a quantitative method to determine which option provides the better outcomes based on current evidence.[56]
Therefore, in this study, we determined, using decision analysis, which bisphosphonate provides the better outcome for prevention of osteoporotic fractures, in terms of quality of life.
METHODS
1. Model design
A decision tree, depicting the probabilities and outcomes (utilities) of each bisphosphonate for the prevention of osteoporotic fracture in postmenopausal women, was developed using decision analysis software (TreeAge Pro 2011; TreeAge Software Inc., Williamstown, MA, USA).
In root node, that is a small square on the left side and represents the first set of decision alternatives, postmenopausal women face a choice; which bisphosphonate is administrated or not to them. In the model, moving from left to right, the tree divides to branch at chance nodes, each of which represents an opportunity for a patient to enter into one or more health states (well, vertebral fracture, or hip fracture) after an administration. Each terminal node of the tree has a corresponding health state and has an associated utility value (Fig. 1).
2. Event probabilities
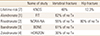
We conducted a literature review to identify baseline probability estimates for each chance node. Among original studies which included outcomes to prevent vertebral and hip fracture in postmenopausal women during at least 1-year follow-up, early RCTs with placebo were selected, because there was no study with head-to-head comparison. Finally, 4 original articles were selected for each bisphosphonate.[1234] The percentage of reduced risk of vertebral fracture and hip fracture were reviewed (Table 1).
For probability of vertebral fracture and hip fracture in decision tree, the lifetime risks at 50 years old in Korea were used.[7]
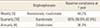
To obtain the whole efficacy of reducing the risk of osteoporotic fracture, the patients should take the medication for a whole year. However, unlike RCTs, the compliance on bisphosphonate was not 100% in real world. The compliance on bisphosphonate has been well known to depend on interval of medication.[89] After the interval of medication was categorized with weekly, quarterly, and annually administration, additional literature review was performed to obtain probability of compliant use for each bisphosphonate in real world (Table 2).[8910]
3. Health utilities
Quality of life after each event was used as utilities in decision tree. Quality of life were determined in consensus committee, which included 3 orthopedic surgeons with 24 (KHK), 16 (YCH), and 8 (YKL), years of experience. Quality of life on a scale ranged from 0 (death) to 1.0 (perfect health). Hip fracture was defined as a score of 0.3, and vertebral fracture for 0.5 in consensus committee.
4. Statistical analysis
TreeAge Pro 2011 (TreeAge Software Inc.) was used to construct the decision analysis. Final quality of life was calculated using a "roll back" technique, and sensitivity analysis was conducted to assess the uncertainty of the decision tree model. Threshold values were defined as point of intersection at which preferred bisphosphonate changed. The variables with greatest uncertainty were the probabilities of compliance of bisphosphonate. The probabilities of compliance of ibandronate ranged from 56.6% to 82.8% (Table 2).[10]
This study was exempted from institutional review board (IRB) review because it did not involve human subjects.
RESULTS
When performing the roll back, the expected values for risedronate, Ibandronate, and zoledronate were 0.75, whereas the expected values for alendronate were 0.71. Meanwhile the expected values of no treatment were 0.67. Accordingly, the decision model showed that risedronate, ibandronate, and zoledronate was the better than alendronate in terms of quality of life.
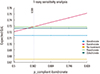
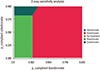
In addition, one-way sensitivity analysis on the probabilities showed that ibandronate was superior to another bisphosphonates, when the probability of compliance on ibandronate was more than 0.589 (Fig. 2). Two-way sensitivity analysis on compliance on ibandronate and zoledronate showed that bisphosphonate with higher compliance was superior to another bisphosphonate, when the probability of compliance was more than 0.589 (Fig. 3).
DISCUSSION
On the decision analysis model presented that bisphosphonate with higher compliance is a better choice than another bisphosphonate in terms of quality of life. Key factor is compliance of each bisphosphonate in this study. Furthermore, the sensitivity analyses showed that our decision model was relatively stable.
Although the efficacy of each bisphosphonate in elderly patients have been previously reported,[1234] the study does not provide a decision guide due to a lack of uniform clinical outcome measures. In the present study, the quality of life was used to unify the clinical outcomes of each scenario.
Poor compliance is a key-limiting factor in treatment of osteoporosis, which is asymptomatic silent chronic disease until osteoporotic fractures occur.[1112131415] Higher age, low socioeconomic status, poor awareness on osteoporosis, complex method of ingestion and adverse effect such as gastroesophageal irritation have been well-known risk factors for low compliance with bisphosphonate.[161718]
New type of bisphosphonate with various dose intervals have introduced to overcome poor compliance, and bisphosphonates with longer interval showed higher compliance.[8919]
Although several types of bisphosphonate have been presented to have higher efficacy to prevent osteoporotic fracture, compliance on it was revealed to be key factor in this decision analysis study.
Although decision analysis is a useful tool to apply evidence-based medicine to make informed clinical decisions, the obtained results depend on the level of the selected studies and the validity of the used utilities in the model.
Several limitations of the present study should be considered. First, the utilities used in this study, which were physicians-derived, need to be validated with respect to their values to patients and the clinical meaning of utility differences. Second, for reason of simplicity, our model included only vertebral and hip fracture, despite the fact that other osteoporotic fractures could also affect quality of life. Third, compliance might be more diverse than those included in this study, and such considerations could alter expected clinical outcomes. To overcome these limitations, we conducted sensitivity analyses with a broad range of clinically pertinent values, which presented the relatively stability of our decision model. Fourth, we did not include another type of bisphosphonate such as combination with vitamin D.
Despite these limitations, the present study presented that compliance play a key role for better quality of life in treatment of osteoporotic patients, regardless type of bisphosphonate.

 XML Download
XML Download