

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In 1989, Rosenberg reported that no decline with age is more dramatic or potentially more functionally significant than the decline in lean body mass and proposed the term "sarcopenia" to describe the age-related decrease in muscle mass.[1] Since then, the implications of loss of age-related skeletal muscle mass have attracted increasing attention. These age-related changes are a major cause of impaired physical functioning in older adults and contribute to limited mobility, falls, osteoporosis, and hospitalization.[234] Moreover, it has now clear that skeletal muscles are also involved in endocrine and metabolic activities, such as glucose, glycogen, and lipid metabolism.[5] Therefore, sarcopenia have been widely investigated in a variety of fields.
Despite the clinical importance of sarcopenia in the elderly, the criteria for defining and clinically diagnosing sarcopenia are unclear and vary among studies and experts. Thus, several groups of experts have convened to establish consensus diagnostic criteria for sarcopenia.[678] Although the criteria lack clinical evidence, this is a significant advance, as many studies can now be conducted based on a single criterion without confusion. The Asian Working Group for Sarcopenia (AWGS), which includes Korea, is one of these efforts.[8]
Korea is one of the most rapidly aging countries in the world and a number of studies have focused on the prevalence, etiology, and clinical issues of sarcopenia in Korea. However, the criteria for defining sarcopenia vary among studies. Furthermore, as the distributions of muscle mass and height of Korean women in different age groups differ from those of other countries, confusion has arisen when defining cutoff values. As a result, the prevalence of sarcopenia differs markedly among studies using different definitions of sarcopenia. This study used the AWGS definition for Korean women to determine the prevalence of sarcopenia in Korean.
METHODS
This study was based on data obtained from the 2008 to 2011 Korean National Health and Nutrition Examination Surveys (KNHANES) IV and V, which is a nationally-representative survey conducted by the Korean Ministry of Health and Welfare. These surveys have been conducted periodically since 1998, using a rolling sampling design involving a complex, stratified, multistage, probability-cluster survey of a representative sample of the non-institutionalized civilian population to assess the health and nutritional status of the Korean population. Whole body dual energy X-ray absorptiometry (DXA) scans were performed on individual's ≥10 years old from July 2008 to May 2011. A total of 5,211 women >50 years were included in the study. Written informed consent was given by all participants, and the KNHANES IV and V protocols were approved by the Institutional Review Board of the Korean Center for Disease Control and Prevention.
The whole-body DXA examinations for the KNHANES study were conducted with the QDR4500A apparatus (Hologic, Bedford, MA, USA). The data included values for bone mineral content (g), bone mineral density (BMD) (g/cm2), fat mass (g), lean mass, including bone mineral content (g), and fat percentages of the whole body and for specific anatomical regions. Appendicular skeletal muscle mass (ASM) was obtained by adding the muscle masses of the four limbs, which were calculated by assuming that all non-fat and non-bone mass is skeletal muscle.[910] The skeletal mass index (SMI) was defined as ASM/height2.[910] The AWGS adopted a classical approach to determine the cutoff value by using the value two standard deviations below the mean for a young reference group, which was 5.4 kg/m2 for women. We used 5.4 kg/m2 as the cutoff value to determine prevalence for sarcopenia among Korean women.[8]
RESULTS
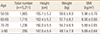
The 2008 to 2011 KNHANES involved 5,211 women >50 years. The age distribution was 1,965 in their 50s, 1,715 in their 60s, 1,236 in their 70s, and 295 ≥80 years. Mean height and weight decreased with age. SMI increased slightly from the 50s to 60s and then decreased with age (Table 1).
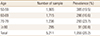
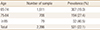
The prevalence rates of sarcopenia using the 5.4 kg/m2 cutoff value were 385 (19.5%) for women in their 50s, 286 (16.6%) for women in their 60s, 293 (23.7%) for women in their 70s, and 91 (30.8%) for women ≥80 years (Table 2). The prevalence rates of sarcopenia were 307 (19.0%) for women 65 to 74 years, 194 (27.4%) for women 75 to 84 years, and 32 (40.5%) for women ≥85 years (Table 3). The overall prevalence among women >50 years was 20.2%. The prevalence of sarcopenia was 22.1% in women >65 years.
DISCUSSION
The definition of sarcopenia varies. Baumgartner et al.[10] suggested a height squared adjusted index, Janssen et al.[11] suggested a weight adjusted index, and Newman et al.[12] suggested a fat mass adjusted index. Furthermore, several methods have been used to determine the cutoff value, such as using the value 1 or 2 standard deviations below the mean of healthy adults or using the lowest quintile of a study population.[1314] As a result, the prevalence of sarcopenia can vary depending on the method used.[71115] As interest in the endocrine role of muscle has increased, many studies have investigated the associations between sarcopenia and other clinical parameters, such as obesity and BMD.[1617] The results of these studies differ depending on the method used.[15]
To clarify the definition of sarcopenia, various working groups have published consensus papers. Our study is the first to address the prevalence of sarcopenia using 5.4 kg/m2 as recommended value by the AWGS in Korea. Various studies about sarcopenia have been released in Korea.[1819] However, different definitions were used in each study.[1819] This phenomenon is prominent in Korea because the differences in height between age groups is greater among Koreans compared with those in other countries.[202122] This large difference limits use of the height adjusted index. Using the height adjusted index results in a very low prevalence of sarcopenia in Korea. Thus, many studies chose to use a weight adjusted index. The prevalence of sarcopenia was 0.1% when using the height adjusted definition and 9.7% when using the weight adjusted definition in a study on the prevalence of sarcopenia using KNHNES data.[18] Another study, which was part of the Korean Sarcopenic Obesity Study, reported sarcopenia prevalence of 4.1% using the height adjusted index and 14.2% using the weight adjusted index.[19]
Our results show that overall prevalence of sarcopenia was 20.2% in women ≥50 years and 22.1% in women ≥65 years. We assumed that women >50 years were postmenopausal and that women >65 years were elderly. The prevalence of sarcopenia in this study is relatively high than other studies.[23] The reason is might be related with difference of definition and characteristics of cohort.[15] Our study had several limitations. First, we only considered low muscle mass when defining sarcopenia regardless of muscle function. Second, we did not specifically exclude women with a metabolic disease, such as hyperthyroidism or diabetes mellitus, which can influence lean body mass.
Although the prevalence rates we obtained have little clinical relevance because the cutoff was not calculated using our own cohort, the value we obtained was within the range of other studies about sarcopenia.[101218242526] Furthermore, using the 5.4 kg/m2 cutoff was useful to compare with other studies about sarcopenia in Korea.
 XML Download
XML Download