

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
There has been growing concern worldwide regarding health problems resulting from exposure to heavy metals, such as lead, mercury and cadmium. Because toxic heavy metals such as lead, mercury and cadmium are widely dispersed in the environment,[123] members of the general population, not only those in contaminated areas, are exposed to low doses of heavy metals during their lifetime. These heavy metals are accumulated in the human body due to no mechanism for active excretion of toxic heavy metals.[4]
Long-term exposures of heavy metals are known to associate with development and progression of bone disease.[567] Although pathogenic mechanisms of lead, mercury and cadmium are still investigating, these heavy metals are toxic to the human body by increasing oxidative stress. This mechanism is possible to explain the relationship between exposure of heavy metals and various metabolic disorders such as hypertension and diabetes.[8] Toxic heavy metals also are known to relate with increasing the risk of osteoporosis.[910111213] Several studies demonstrate that osteoporosis and sarcopenia have similar pathophysiology and risk factors. Therefore, long-term accumulations of these heavy metals may be related with bone and muscles weakness.
Recently, sarcopenia in the elderly is representative disease in muscular changes and an independent risk factor for falls, disability, morbidity, and mortality.[14151617] As pathophysiologic mechanisms, sarcopenia generally results from a complex bone-muscle interaction in relation to chronic disease and aging. However, there was no report to study relationship of heavy metals and sarcopenia.
Therefore, the purpose of this cross sectional study was to assess the relationship of blood lead, mercury and cadmium levels with sarcopenia and their cumulative effect on skeletal muscles in elderly populations using Korea National Health and Nutritional Examination Surveys.
METHODS
1. Ethics statement
This study's protocol for analysis of the 2008-2011 Korea National Health and Nutritional Examination Surveys (KNHANES) data was reviewed and approved by the Institutional Review Board (Approval No. 2008-04EXP-01-C, 2009-01CON-03-C, 2010-02CON-21-C and 2011-02CON-06-C) of the Korea Centers for Disease Control and Prevention (KCDC). Informed consent was obtained from all of the participants when the 2008, 2009, 2010, and 2011 KNHANES were conducted.
2. Participants
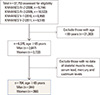
This study was based on data from the KNHANES 2008-2011, which was conducted by the Korea Ministry of Health and Welfare. KNHANES is a nationwide representative cross-sectional survey for the Korean population with a clustered, multistage, stratified, and rolling sampling design. KNHANES comprises three sections: a health interview, a health examination, and a dietary survey. The survey data are collected via household interviews and by direct standardized physical examinations conducted in specially equipped mobile examination centers. We collected data from 37,753 participants from 2008 (n=9,744), 2009 (n=10,533), 2010 (n=8,958), and 2011 (n=8,518). Participants were excluded if they were under the age of 65 years, or if data were not available to evaluate skeletal muscle mass, and serum lead, mercury and cadmium levels. After these exclusions, a total of 704 participants (males 344, females 360) were analyzed in the present study (Fig. 1).
3. Health examination survey
A health questionnaire was used to obtain information on age, gender, socioeconomic status, educational status, smoking status (current, former, or never smoker), alcohol intake and moderate physical activity and walking activity (yes or no). Moderate physical activity was 5 or more days of moderate-intensity activity for at least 30 min per day. Walking physical activity was 5 or more days of walking for at least 30 min per day. Body weight and height were measured in light clothing with no shoes, and body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Information on diabetes as a potential confounding factor was examined through the health interview survey.
4. Measurement of lead, mercury and cadmium levels in whole blood
We measured total lead, mercury and cadmium levels in blood. For measurements of blood heavy metal levels, blood samples of individual subjects were collected in standard commercial evacuated tubes containing sodium heparin (Vacutainer; Becton, Dickinson & Co, Franklin Lakes, NJ, USA). Graphite-furnace atomic absorption spectrometry with Zeeman background correction (AAnalyst 600; Perkin Elmer, Wilton, CT, USA) was used for measurement of blood lead and cadmium levels. A gold-amalgam collection method with a DMA-80 (Milestone, Sorisole, Italy) was used for measurement of blood mercury levels. All blood metal analyses were performed at the Neodin Medical Institute, a laboratory certified by the Korean Ministry of Health and Welfare.
5. Measurements of appendicular skeletal muscle mass and definition of sarcopenia
Body composition was measured by whole-body dual energy X-ray absorptiometry (DXA; QDR 4500A, Hologic Inc., Bedford, MA, USA). Bone mineral content, fat mass and lean soft-tissue mass were measured separately for each part of the body, including the arms and legs. The lean soft-tissue masses of the arms and legs were almost equal to the skeletal muscle mass. As absolute muscle mass correlates with height, the skeletal muscle mass index was calculated by the following formula: lean mass (kg)/height2 (m2), which is directly analogous to BMI (weight [kg]/height2 [m2]). Arm skeletal muscle mass index was defined as (arm lean mass [kg]/height2 [m2]). Leg skeletal muscle mass index was defined as (leg lean mass [kg]/height2 [m2]). Appendicular skeletal muscle mass index (SMI) was defined as the sum of the arm SMI and the leg SMI. Sarcopenia was defined according to the criteria for the Asia Working Group for Sarcopenia (AWGS) (SMI <5.4 kg/m2 in females and <7.0 kg/m2 in males).[18]
6. Dietary intake measurement
Dietary intake was assessed by trained staff using a complete 24-hr recall method. Daily intake of energy and protein were calculated by referencing nutrient concentrations in foods according to the Korean Food Composition Table.
7. Biochemical analyses
Blood and urine samples were collected the morning after fasting for at least 8 hr. Collected samples were immediately refrigerated and transported in cold storage (4℃-8℃) to the central laboratory of Neodin Medical Institute (Seoul, Korea) within 24 hr. Transported samples were separated into small aliquots and stored at -70℃.
Serum 25-hydroxy-vitamin D (25-[OH]D), parathyroid hormone, and alkaline phosphatase levels were measured using a gamma counter (1470 Wizard; Perkin Elmer, Turku, Finland), Hitachi Automatic Analyzer 7600 (Hitachi Ltd., Tokyo, Japan) and LIAISON (DiaSorin, Stillwater, MN, USA) with radioimmunoassay (25-hydroxy-vitamin D 125I RIA Kit; DiaSorin), enzymatic (Pureauto S ALP; Sekisui Medical Co., Ltd, Tokyo, Japan) and chemiluminescence immunoassay (N-tact PTH Assay kit; DiaSorin), respectively.
8. Statistical analysis
Complex sample analysis was used in this study to correct the distributions of the cluster sample regarding the primary sampling unit, covariance and significance to correspond with those of the general Korean population. All analyses were carried out using the sample weights of KNHANES.
To compare means between the non-sarcopenia and sarcopenia groups, Student's t-test was used and to compare proportions, the χ2 test was used. Multiple logistic regression analysis was conducted to calculate odds ratio and 95% confidence intervals (Cis) for the association between frequency of binge drinking and the presence of sarcopenia after adjustment for demographic variables (age, waist circumference and BMI), which served as covariates. Spearman correlation analysis was performed to investigate the association between heavy metals and variables. The geometric means with standard errors of heavy metals were calculated according to their quartiles. For each heavy metal, subjects were categorized into quartiles. To evaluate the cumulative effect of the three heavy metals, each heavy metal was categorized into 10 groups using the 10th percentiles. The category number of each heavy metal (1-10 assigned to successively increasing categories) was added to make the sum of heavy metal levels, producing a value of 3 to 30, which was itself categorized into quartiles, generating four groups.
Multivariate logistic regression analysis was used to calculate individual heavy metals or sum of heavy metal effects on sarcopenia, adjusting for BMI, waist circumference, and energy intake. All statistical tests were two-tailed, and statistical significance was defined as P<0.05. The statistical analysis was performed using SPSS 22.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Baseline characteristics of elderly populations according to the presence of sarcopenia
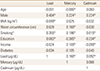
Seven hundreds four persons (344 in male and 360 in female) were enrolled in this study. The mean age were 70.5 years (range, 65-87 years) in male and 72.5 years (range, 65-85 years) in females. Prevalences of sarcopenia were 26.7% (92/344) in male and 7.5% (27/360) in female and baseline values for the elderly populations according to the presence of sarcopenia are shown in Table 1 and 2. BMI (P<0.001), waist circumference (P<0.001), and appendicular SMI (P<0.001) differed significantly between non-sarcopenia and sarcopenia in both genders. Mean serum levels of lead in sarcopenia group were significantly higher than non-sarcopenia males (P=0.03).
2. Correlations of lead, mercury and cadmium levels with clinical variables
Most variables showed correlations with lead, mercury and cadmium levels. Males showed higher concentrations of blood lead, mercury and cadmium than females. Smoking was closely correlated with blood lead (r=0.355) and mercury (r=0.196) levels. Correlations were observed among the three heavy metals: r=0.160 and r=0.092 for lead and mercury, lead and cadmium, respectively (Table 3).
3. Prevalence of sarcopenia according to heavy metal category
When no variable was adjusted, the prevalence of sarcopenia increased with increasing lead concentration category. However, the prevalence of sarcopenia decreased with increasing mercury and cadmium concentration category.
In male, after adjustment for BMI and waist circumference, odds ratios were increased with increasing lead (P=0.005), mercury (P=0.001) and cadmium (P=0.010) concentration. However, the sum of heavy metals showed no association with the prevalence of sarcopenia (Table 4).
In female, after adjustment for BMI, waist circumference and energy intake, the odds ratios were increased with increasing concentration category of lead (P<0.001), mercury (P<0.001) and cadmium (P<0.001), and the sum of the three heavy metals (P<0.001) (Table 5).
DISCUSSION
Accumulations of heavy metals in human body are known to cause of public health problems. Of heavy metals, lead, mercury and cadmium are representative toxic metals and related researches have been reported. This study shows that odds ratio for sarcopenia, after adjustment, were increased with concentration category of lead (P=0.005 and P<0.001), mercury (P=0.001 and P<0.001) and cadmium (P=0.001 and P<0.001) in males and females, respectively. Therefore, we found that elderly populations with sarcopenia had high serum levels of heavy metals in both genders.
Recently, sarcopenia, which is defined as the age-related decrease in muscle mass, have been widely investigated in a variety of fields because sarcopenia is known to a major cause of impairment of physical function, limitation of mobility, falls, osteoporosis, and hospitalization.[141516171920] Although its cause is not completely understood, sarcopenia generally results from a complex bone-muscle interaction in relation to chronic disease and aging.[212223] Therefore, effects of heavy metals in bone metabolism are also important to muscular metabolism in elderly populations.
Of three representative heavy metals, relationship between bone metabolism and lead are well established, which is accumulated more than 90% of lead in bone.[2425] Several human studies have demonstrated that lead interfered with bone formation and bone strength and increase the risk of osteoporosis and bone fracture.[26272829] Campbell and Auinger [30] reported negative association between lead exposure and BMD and resulted in osteoporosis in adult humans using data from the Third National Health and Nutrition Examination Survey (NHANES III) in the USA. Several animal studies confirmed that lead affects osteoblast and osteoclast function.[11313233] In addition, mercury influences calcium metabolism and affects bone.[10] Suzuki et al. [34] conducted an animal study to examine the effects of heavy metals such as cadmium and mercury on calcium homeostasis, plasma calcium and calcitonin in goldfish. They found that mercury influenced calcium metabolism and affected bone. However, effect of Mercury in bone metabolism are still controversial.[35]
Recently, exposure to cadmium has attracted increasing attention as a risk factor for osteoporosis. Wallin et al.[13] examined the associations between low-level cadmium exposure, from diet and smoking, and BMD and incident fractures in 936 elderly males from the Swedish cohort of the Osteoporotic Fractures in Men (MrOS) study. They found that even a relatively low cadmium level increases the risk of low BMD and osteoporosis-related fractures in elderly males. Engström et al.[9] investigated the association between low environmental cadmium exposure and BMD and fracture risk in 2,688 elderly females using a Swedish Mammography cohort. They found that long-term, low-level exposure to Cd from food (mainly cereals, vegetables and potatoes), is associated with a higher risk of osteoporosis and fractures. Chen et al.[36] found a strong relationship between blood Cd level and decreased BMD, especially in females. In addition, they determined that blood Pb level might be related to low BMD in males. They suggested that Cd and Pb might have an interactive effect on bone.
These effects of bone metabolism by accumulations of three heavy metals in human body are also affect in muscular mechanism and resulted in sarcopenia. Although no direct study between toxic heavy metals and sarcopenia has been conducted, the findings of this cross sectional study might be one of explanations of relationship between heavy metals and sarcopenia.
This study had several limitations. First, it did not evaluate the causality between heavy metal exposure and sarcopenia. Prospectively designed studies are mandatory to clarify this relationship. Second, because blood levels of lead, mercury and cadmium differ among ethnic groups, this result might not be able to be extrapolated to other ethnic groups. Third, although lead, mercury and cadmium levels in blood are widely used and well-established biomarkers of exposure, and those blood concentrations may be correlated with chronic accumulated exposure in the general population with stable environmental exposure to heavy metals, they reflect mainly recent exposure. Therefore, they could underestimate cumulative exposure. In particular, we measured total mercury only in whole blood, including both the inorganic and organic forms, without differentiating other forms of mercury. Although total mercury in blood may be a reliable biomarker of mercury exposure, we could not infer which form is the major contributor to blood mercury and by which route exposure occurs. Fourth, we did not measure all environmental exposure to heavy metals; thus, the possibility of a positive relationship between other heavy metals with sarcopenia remains. Therefore, the relationship between heavy metals and sarcopenia should be verified in further longitudinal studies. Finally, although a definition of sarcopenia has been established, debate is ongoing. We used the definition of the AWGS group.[18]
In conclusion, this study demonstrates that high levels of blood lead, mercury and cadmium increase the prevalence of sarcopenia in both genders of elderly populations.




 XML Download
XML Download