

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Various senile diseases have become a big problem as aging of population is under progress these days. In the case of musculoskeletal diseases, the prevalence rate of osteoporosis has increased. Consequently, osteoporosis triggers the risk of spine and other bone compression fracture. Thus, the critical characteristics of osteoporosis are becoming a big issue.
World Health Organization (WHO) defines osteoporosis as "A systematic skeletal disease that is characterized by decrease in bone density and abnormality in bone structure, which results in the bone to become weak and easily breakable".[1]
The prognosis of patients who have been diagnosed with osteoporosis is grim as osteoporosis is a major risk factor for hip joint, spine, and radio-ulnar joint.[2]
Therefore prevention is the most important factor in osteoporosis.
Osteoporosis has many risk factors but one of the factors related to drugs is the dose of selective serotonin reuptake inhibitors (SSRI).[3] It is known that the said drug effects the circulatory system to induce low blood pressure and increase the possibility of syncope. This increases the danger of falling and the probability of stress fracture in patients who take regular doses of SSRI.[4-8] But many doctors clinically underestimate the negative effects of SSRI compared to other risk factors of osteoporosis and fracture. At the same time, there is a serious lack of thesis on the correlation of SSRI and osteoporosis. Thus, this thesis targeted 5 of Korea's veterans hospital and investigated the reality of osteoporosis check through bone mineral density (BMD) of patients taking SSRI.
METHODS
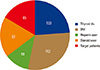
From January 1st of 2011 until March 1st of 2013, we selected 526 patients from 5 veterans hospital in Korea who took the SSRI for more than 2 months. Of those patients, we excluded patients who were prescribed medicine for thyroid disease, diabetes mellitus (DM) underlying disease or took heparin, and steroid, which are also known risk factors of osteoporosis. After the exclusion, we ended up with 85 patients (Fig. 1). At this point, we investigated the number of patients who has gone through BMD check at least once during the investigation period. The method that the 5 veterans hospital used for their bone densitometry was dual energy X-ray absorptiometry (DXA), which fixes the measurement location of the patient as constant and quantify the bone density of lumbar vertebra no.2, no.3, and no.4.
Since this research applied the retrospective method, we only asked approval from a portion of patients.
RESULTS
Of the 526 patients who were selected for our research, the average age of 85 patients, who were not prescribed medicine for thyroid disease, DM underlying disease or took heparin, and steroid, was 68.4 years. The ratio of men to women was 1:3.47. Out of the 85 patients who took SSRI, 71 patients were diagnosed with major depression disorder, 10 patients were diagnosed with generalized anxiety disorder, and 4 patients were diagnosed with obsessive compulsive disorder and were at the time of writing, under medical treatment by the department of neurology. Only 34 patients out of 85 patients confirmed BMD check through orthopedics or hospitalization. Only 3 patients implemented more than 1 BMD check and the average BMD result for the patients showed a T-score of -2.8.
1. Consideration
As the population of seniors increase, there is much attention on senile fracture or osteoporosis related fractures. The 'Korea Health Statistics 2009' implemented a bone densitometry, which measured the lumbar vertebra and proximal femoral. According to this report, the prevalence rate of osteopenia was 47.5% and the prevalence rate of osteoporosis was 23.1% for those aged over 50. For those aged over 65, the prevalence rate of osteopenia was 42.1% and the prevalence rate of osteoporosis was 42%.
But the recognition rate of osteoporosis was 26.4% and the treatment rate was 12.7% which is a comparatively low level compared to other chronic illnesses.[9] Furthermore, among various risk factors of osteoporosis, there have been studies that report that the increase of concentration of serotonin by the serotonin reuptake inhibitors lead to a decrease in bone density. Serotonin takes effect on the 5-hydroxytryptamine receptor 1b (Htr1b), which is manifested in the osteoblast, and it is known that one of the functions of serotonin is that it suppresses the proliferation of osteoblasts that eventually increase the danger of osteoporosis for patients taking SSRI.[10,11] It is explained that the bone density is decreased through the mechanism of the serotonin receptor and carrier, that is usually limited to osseous tissue affecting, the physiologic structure of the bone.[4]
In case of adults, the life prevalence rate of depressive disorder was 3.3-5.6% and the point prevalence rate were within 2%. In case of the elderly, the life prevalence rate of depressive disorder was higher than adults with the statistic of 5.4%-7.5%. In the research that simultaneously investigated the prevalence rate of depressive disorder ranging from adults to elderly, the total prevalence rate was 3.6%. But those aged over 65 scored a high mark of 4.6% on prevalence rate.[12] Considering the rapid aging of the Korean population, a continual increase in patients with depressive disorder is anticipated, and patients who take SSRI are expected to increase accordingly. SSRI selectively inhibits the reuptake of serotonin and doesn't have much effect on the norepinephrine, dopamine, anti-choline.[13] More than half of the patients do not suffer from side effects. Also, the drug interruption rate due to side effects are much smaller than tricyclic antidepressant (TCA) so it is widely used as the basic drug for depressive disorder and anxiety disorder.[13-15] As the prevalence rate of patients who suffer major depressive disorders is expected to increase, an increase in number of patients taking SSRI is anticipated in the future as well.
But this information is not well-known to many doctors who practice clinical medicine. Also it is rare to find any thesis relating to this subject done through research using an orthopedic approach. Judging by the research done in this paper, insufficient amount of discrimination and prevention is common. Therefore, keeping in mind that the aging society will continue on its way, it is necessary for Korea to make sure that patients who take SSRI for a long period of time receive bone densitometry.
A selection bias inevitably occurred in this thesis as we lacked diversity in selection of patients since the selection was based on 5 of the veterans hospital in Korea. Another limitation would be that we couldn't implement long-term investigation on the number of patients taking SSRI who implemented BMD check. Lastly there needs to be further research on the matter of additional examination such as bone turnover marker as well as BMD check.
DISCUSSION
Insufficient amount of discernment examination such as regular BMD check for patients taking SSRI for a long time is taking place while the fast aging of population and the expected increase in neurology patients remain imposing.
By implementing long term prevention and treatment of osteoporosis for patients who took SSRI for a long time, we would be able to cut medical costs as well as extend the average life span, which will eventually contribute to the increase in quality of life.
 XML Download
XML Download