

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stress fractures can be divided into fatigue and insufficiency fractures.[1] A fatigue-type stress fracture occurs when abnormal or repeated stress is applied to normal bone, whereas an insufficiency-type fracture is produced by normal stress on abnormal bone such as when there is impaired bone structure. Insufficiency fracture patients are older, typically postmenopausal women with osteoporotic bones.[2] The risk factors are the same as those of osteoporosis, and also include abnormal bone conditions which affect bone turnover such as Paget's disease, osteomalacia, diabetes mellitus, hyperparathyroidism, chronic renal failure, high-dose glucocorticoid therapy, and rheumatoid arthritis.[3] The most common sites of insufficiency fractures are the vertebrae, sacrum, pelvic rami, and femoral neck.[4] Less often, the lower leg and foot are involved, with the common sites being the distal tibia, calcaneus, metatarsal, and talus.[5-7] However, reports of a medial malleolar insufficiency fracture without a history of trauma in elderly patients is extremely rare and it has not been reported in Korea up until now. Thus, we report a case with medial malleolar insufficiency fracture of the ankle in an elderly patient with osteoporosis that was treated with percutaneous screw fixation after there was no symptom improvement with conservative treatment.
CASE
A 65-year-old female patient presented with left ankle pain of 2 months' duration. There was no history of trauma or bisphosphonate use for osteoporosis and the pain was activity-related and relieved partially by rest or elevation. In the past medical history, no special diseases such as diabetes, hypertension, and cerebrovascular diseases were present and she was a non-smoker and a non-drinker. The physical examination showed mild localized tenderness in the medial aspect of the ankle and no swelling. The range of motion of the ankle was full, and stability was intact. She was 157 cm in height, had a body weight of 58 kg, and her body mass index was 23.5 kg/m2. The bone mineral density (BMD) was measured utilizing peripheral quantitative computed tomography (P-QCT; Somatom sensation 16, Simens, Erlangen, Germany). On assessment of the results, severe osteoporosis was considered because the BMD and T-score of the lumbar vertebrae (L1-4) were 40.4 mg/cm3 and -4.31 (Fig. 1). At the time of visiting, a plain radiograph of the left ankle showed a fracture that was not clearly depicted but showed as a faint vertical sclerotic line in the medial malleolus of the ankle joint (Fig. 2A). She was treated with restriction of activity and non steroidal anti-inflammatory drugs (NSAIDs). After 3 weeks of treatment, she still had pain in the left ankle. Magnetic resonance imaging (MRI) was performed. The MRI of the left ankle revealed an irregular vertical low signal line with surrounding marrow edema at the junction of the medial malleolus and the tibial plafond which did not extend to the medial malleolar cortex of the tibia (Fig. 2B, 2C). We diagnosed a medial malleolar insufficiency fracture of the ankle.
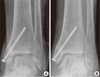
An operation was performed because of progressive pain and difficulty of ambulation during the follow-up, leading to early recovery and normal activities. The patient was placed in the supine position under spinal anesthesia. The fracture was internally fixated with a percutaneous cannulated screw under c-arm guidance (Fig. 3A) and at the same time an arthroscopic procedure was performed. The arthroscopic examination revealed no displacement of the medial fracture line within the joint but synovitis was observed. Arthroscopic debridement was performed. After surgery, she was kept in a non-weight bearing cast for 5 weeks. At the fifth week, she was allowed to perform ankle range of motion exercises and partial weight-bearing walking. As of the 4-month follow-up, there was bony union and she had recovered to full activity with the treatment including osteoporosis medications (Fig. 3B). The patient was informed of this report.
DISCUSSION
Insufficiency-type stress fractures affect abnormal bone that is exposed to stresses that normally would not be sufficient to cause mechanical failure and thus they are often observed in postmenopausal osteoporotic women.[2] The cause of insufficiency fractures is often multifactorial, and typically the main factor is osteoporosis followed by osteopenia. Osteopenia decreases bone elasticity enough to allow fractures to occur from normal activity; however, according to Breer et al.[8], the stress fracture incidence in elderly patients seems to be multifactorial and not based on osteoporotic changes alone. Also, balanced calcium and vitamin D metabolism seems to be of paramount importance in the prevention of insufficiency fractures in elderly patients.[8] The reason why osteoporosis leads to insufficiency fractures remains unclear, but in this case, severe osteoporosis was considered a cause of the insufficiency fracture. Although the defined mechanisms are unclear, insufficiency fractures mainly occur in the medial malleolus of the ankle when a physiological torsional load is applied to the bone, or a muscular contracture, or a misalignment force such as occurs with a sprained ankle impacts bone that has inadequate mechanical strength.
The diagnosis of an insufficiency fracture is primarily based on the history and physical examination. The leading clinical symptoms in patients with an insufficiency fracture is pain, and this may be worse with loading and increased physical activity.[9] Radiographs are still the most widely used imaging methods for identification of insufficiency fractures, but the sensitivity is limited. MRI is the diagnostic agent of choice due to its higher sensitivity and specificity, and it allows the differentiation of benign versus malignant fractures.[10] The typical MRI appearance of an insufficiency fracture is a low marrow signal and prominent enhancement on T1-weighed images and a high marrow signal with extension into adjacent soft tissue on T2-weighed images. An early diagnosis is best made with a bone scan or an MRI, as radiographs may initially appear normal. In this case, the clinical signs were mild pain in the medial aspect of the ankle, which was confirmed by an MRI.[11,12] The treatment of an insufficiency fracture depends on the clinical presentation and whether the fracture is complete or incomplete. Treatment options are conservative treatment, a splint or a cast, and an operation such as internal fixation. Also, treatment of the underlying cause of bone weakness is essential.[2,3]
We experienced a rare case of medial malleolar insufficiency fracture of the ankle that was related to severe osteoporosis in an elderly patient. Medial malleolar insufficiency fracture of the ankle is easily overlooked unless it is suspected. When ankle pain becomes suddenly exacerbated in postmenopausal elderly patients, insufficiency fractures should be considered, and if they are present, diagnosed with a bone scan or an MRI.


 XML Download
XML Download