

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The ability to grip is one of the most important functions of the hand, and grip strength can be used to reflect overall muscular strength.[1] Several studies have shown that grip strength is inversely associated with all-cause mortality, functional impairments, frailty markers, cognitive impairments, physical disabilities, and nutritional status.[2-4] One example of using grip strength is the assessment of 'sarcopenia', which is characterized by progressive and generalized loss of skeletal muscle mass and strength with decreased physical performance.[5] Although lower extremity muscle strength is more relevant than upper extremity in terms of gait and physical function, grip strength has been widely used for assessing sarcopenia because it correlates well with lower extremity muscle strength.[6] Furthermore, grip strength measurement is simple and cost-effective.
Grip strength has been found to be associated with numerous factors such as demographics (age, gender), body construct (height, weight, bone mineral density [BMD], hand size, upper arm circumference, hand dominance), socioeconomic variables (occupation, social status, lifestyle) and physical and psychosocial variables. Furthermore, grip strengths significantly differ between ethnicities.[6-18] Although there are a few studies that have assessed normative hand grip strength in Koreans,[19] few studies have looked at comprehensively those factors that potentially affect grip strength in a population-based cohort regarding elderly Koreans. The aim of this study was to evaluate potential factors influencing grip strength in elderly Koreans.
MATERIALS AND METHODS
1. Subjects
This study was conducted as a substudy of the Korean Longitudinal Study on Health and Aging (KLoSHA). The KLoSHA was designed as a population-based prospective cohort study of health, aging, and common geriatric diseases in the elderly Korean population, conducted from September 2005 to August 2006, and involved residents of Seongnam City, a satellite of metropolitan Seoul, South Korea. The institutional review board of the authors' hospital approved this cohort-based study, and written informed consent was obtained from every participant. Candidates were randomly drawn from a roster of patients 65 years or older using a computer-generated list of resident registration numbers. We invited 1,118 individuals to participate in this study by letter and telephone, of which 696 agreed to participate (a response rate of 62.3%). A specially trained nurse recorded demographic data and conducted an interview, asking patients questions regarding a current or past medical history of illness or surgery. Several questionnaires such as general health status, upper and lower extremity functions, cognitive function, depression etc., were used at the point of enrollment. We excluded participants who had a history of trauma in the hand or wrist or prior surgery on the upper extremity. We also excluded those with symptoms of shoulder or elbow pain, and patients with rheumatoid arthritis. Finally, 266 participants (143 males, 123 females) were included in the analysis. The mean age of subjects was 71.7 ± 4.4 years (range, 65-87 years) in men, 70.7 ± 4.5 years (range, 65-86 years) in women.
2. Measurement of grip strength
We evaluated grip strengths of the dominant hand in a standardized manner.[20] In a neutral position of the arm, forearm, and wrist, 2 consecutive attempts with 1-minute intervalswere each measured in kilograms with a Jamar 5030J1 hydraulic dynamometer (Sammons Preston, Bolingbrook, IL, USA). For statistical analysis, we used average values.
3. Measurement of potential factors influencing grip strength
Factors assessed for potential association with grip strength were; 1) demographics such as age and gender, 2) body constructs such as height, body mass index (BMI), and BMD, 3) upper extremity functional status using disabilities of the arm, shoulder and hand (DASH) scores,[21,22] and 4) mental health status using a depression scale (geriatric depression scale Korean version, GDS-K) and the short form-36 (SF36) mental health score.[23-25]
Height and body weight were measured by standard methods. BMI was calculated as weight in kilograms divided by the square of height in meters. The BMD (g/cm2) of the lumbar spine (L2-L4) and proximal femur was measured by dual-energy X-ray absorptiometry (DXA; model DPX, GE-Lunar Corp., Madison, WI, USA). All scans performed on the same machine by the same operator were analyzed with the same software. We used femur neck BMD for statistical analysis; Marin et al.[26] reported that handgrip strength and lean mass were the variables that were best explained by femoral neck BMD.
Upper extremity functional status was assessed by using the Korean version of the DASH scores.[21] DASH is a self-administered, upper extremity-specific questionnaire and contains 30 items: 21 on physical function, 5 on symptoms, and 4 on social role functions. The DASH has been widely used for evaluations of upper extremity functions,[22] and is also well known for its reliability and validity.[22] The DASH provides overall scores ranged from 0 and 100 (a best possible score of 0 and a worst possible score of 100).
Mental health status was assessed using a depression scale (GDS-K) and the SF36 mental health score. The GDS-K, which is a standardized self-questionnaire scores ranging from 0 to 15 (a score of 5 or more indicates depression) were used to specifically assess the influence of depression.[23] The SF36 is commonly used to represent broad aspects of patient-reported general health status, especially regarding musculoskeletal disorders.[24,25] The thirty-six items in the questionnaire are grouped on eight health subscales, and these 8 scales can be combined into two summary measures that provide overall estimates of physical health (physical component summary, PCS) and mental health (mental component summary, MCS). We used only MCS score to assess psychological status in this study.
4. Analysis
Descriptive statistics were calculated to determine the demographic and clinical characteristics of participants. Comparison of variables between male and female was tested by using student t-test. Univariate analyses were performed initially between grip strength and potential factors, and then variables that were significant at P < 0.1 in the univariate analyses as well as those factors deemed clinically important were included in the multivariate analyses. Multiple linear regression analyses with stepwise variable selection were used to assess the relative contributions of factors that influence the grip strength. Multiple linear regression models assess the abilities of explanatory variables to account for variations in response variables while accounting for any confounding between explanatory variables, and produce a statistic called adjusted R2, which reflects the percentage of overall variability in the dependant variable that can be explained by the explanatory variables included in a multiple linear regression model. Statistical analyses were conducted using SPSS for windows version 18.0. (SPSS Inc., Chicago, IL, USA) and statistical significance was accepted for P values of < 0.05.
RESULTS
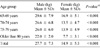
The mean grip strength of dominant hand aged over 65 years was 27.7 ± 7.3 kg in men, and 14.9 ± 5.3 kg in women, and the difference was significant (P < 0.001). In addition, grip strength decreased continuously with further aging in both men and women, as expected (Table 1).
Demographics and other variables assessed for the study subjects are summarized in Table 2. There were significant differences in height, weight, BMD, DASH, GSD-K, and SF36-MCS scores between men and women (Table 2).
As many variables were found to differ between men and women, univariate and multivariate analyses were performed with separating the subjects into both sexes. Univariate analyses demonstrated that age, height, weight, log BMI, BMD, DASH, SF36-MCS, and GDS-K were significantly associated with grip strength of the dominant hand in men. For women, age, height, weight, and BMD were found to be significantly associated with grip strength (Table 3).
In multivariate regression analyses, grip strength was found to be independently associated with age, height and BMI in men, and a model including these factors accounted for 21.3% (adjusted R2 = 0.213, P < 0.001) of the observed variability of grip strength. In women, grip strength was independently associated with age and height, and a model including these factors accounted for 19.7% (adjusted R2 = 0.197, P < 0.001) of the observed variability of grip strength (Table 4).
DISCUSSION
Grip strength has been used as a measure of function in various health-related conditions.[3,15,27] Although grip strength is known to be affected by both physical and psychological factors,[28] few studies have looked at those factors comprehensively in a population-based cohort regarding elderly Koreans. This study demonstrates that in elderly Koreans, grip strength is mainly influenced by age and height in both men and women, and additionally by BMI in men but not in women. BMD or self-reported physical or mental health status was not found to be associated grip strength in elderly Koreans.
There is a consensus that increasing age is inversely related with grip strength, and height correlates with grip strength.[9,29] However, there are contradictory findings regarding association between grip strength and body weight or BMI.[7,29,30] Similar to our findings, Günther et al.[9] found that among arthopometric data, grip strength was correlated best with height in both gender, and weight was associated in men, but not in women in Caucasians. However, Silventoinen et al.[31] reported that grip strength is positively associated with height, weight, and BMI in both sexes in a study of one million Swedish people. Sternfeld et al.[32] reported that there is age-related changes in body composition, particularly increases in fat and central fat deposition and decreases in lean mass, which may result in low skeletal muscle mass and obesity (sarcopenic obesity). Therefore, one can have a high BMI with weak muscle strength due to sarcopenic obesity. Jang[33] reported the prevalence of sarcopenic obesity is 35% in men and 48% in women in elderly Koreans. High prevalence of sarcopenic obesity in women may explain why BMI was not found to be associated with grip strength in women in our study.
It has been suggested that muscle strength may be positively related with higher BMD.[34-36] Bayramoğlu et al.[37] verified that the isometric strength of hip abductors had a significant correlation with femoral neck BMD in postmenopausal sedentary women with and without osteoporosis. Marin et al.[26] also found that grip strength in postmenopausal women was the one that best associated with BMD in all analyzed bone sites. In our study, however, grip strength was not associated with BMDs.
In this study, self-reported upper extremity functional status or mental health status was not found to be associated with grip strength. As we used self-administered questionnaires, we are not able to correlate grip strength with objective test results of physical and mental status. Watson et al.[40] investigated the relationship between grip strength and depression using the Center for Epidemiologic Studies Depression (CES-D) scale, Pain Anxiety Symptoms Scale, and Pain Catastrophizing Scale.[40] They reported that depression scores were minimally associated with decreased hand grip strength and that psychological factors influenced disability (patient-reported health status) more than function (performance-based measures). In contrast, Rantanen et al.[30] demonstrated a stronger association between grip strength and depression using the CES-D scale.
Grip strengths in this study were similar to those reported by Shin et al.[38] These authors examined grip strength data of 924 community-dwelling Korean people aged over 65 years without dementia, and the mean grip strengths were 29 kg in men and 17 kg in women. Grip strengths in Koreans seem to be weaker compared to those in Caucasians (Table 5).[9] Previous studies found ethnic differences in grip strength in association with anthropometric differences,[41-43] and also withmuscle characteristics.[18,44]
A few limitations of the present study require consideration. First, our study focused on elderly Koreans aged over 65 years, but included only small number of participants aged over 80's (3.5% in men, 4.1% in women), which may not represent true elderly population. Second, although we attempted to assess factors influencing grip strength comprehensively, we did not evaluate other factors such as hand size, upper arm circumference, occupation, lifestyle, medications, nutritional status, and other objective physical and mental status measures. Lastly, this is a cross-sectional study, therefore associations found between grip strength and variables may not be causal. A longitudinal study with follow-up grip strength evaluations is required to generalize the findings of this study.
CONCLUSIONS
In conclusion, we found in elderly Koreans without a known history of upper extremity disorder or surgery, grip strength is independently associated with age and height in both gender, and with BMI in men. BMD or self-reported physical or mental health status was not found to be associated with grip strength. This information may be helpful in future studies using grip strength as a measure of function in elderly Koreans.




 XML Download
XML Download