

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The widespread concept of minimally invasive dentistry implies that heavily infected and irreversibly denatured dentin should be selectively removed in order to preserve sound or potentially remineralizable tooth tissue as much as possible.12 Pulp exposure can occur due to the over-excavation of carious lesions,3 while residual caries left on the cavity floor may lead to recurrent caries.4 There are still no widely accepted guidelines to determine how much infected dentin can be left on the cavity floor. Therefore, an accurate method should be selected for the identification and removal of infected dentin layers.
A clinically relevant method for assessing the extent of caries excavation should quantify the remaining infected dentin in the cavity after excavation.5 In the past, culturing methods have been used to quantify bacteria in dentin.6 Hardness has been regarded as a principal criterion for the therapeutic endpoint of caries removal using the conventional excavation method for over 60 years.7 Visualtactile inspection is still accepted as the gold standard for residual caries detection.1 The criterion is that ‘the probe should not stick in the dentin and should not give a tugback sensation’.8 However, probing dental hard tissue can cause iatrogenic pulp injuries and false-positive diagnoses.9
A caries-detecting device known as the fluorescence-aided caries excavation (FACE) device has been recently introduced for the visual detection of residual caries to differentiate infected and affected carious dentin. This device, by visualizing the metabolic products of oral microorganisms known as porphyrins,10 can be beneficial to minimize the risk of caries recurrence.11 When an exposed cavity is illuminated with violet light, the dental hard tissues auto-fluoresce (wavelength, 405 nm), because porphyrins reflect red fluorescence, indicating the required caries excavation locations.12 Sound tissues fluoresce green, while carious tissue fluoresces orange-red with the FACE device. Thereby, the FACE device allows the selective removal of infected dentin and the preservation of non-infected dentin.1314
The aim of the present study was to compare the ability of the FACE device and conventional visual-tactile assessment to detect residual caries in the cavities of permanent teeth, which were prepared by students in grades 4 and 5 and postgraduate students. The null hypothesis was that no difference would be present in the incidence of residual caries detected through FACE device inspection and visual-tactile assessment performed with or without magnifying glasses.
Materials and Methods
Patient selection
A total of 503 non-hospitalized volunteer patients (301 females and 202 males) were selected for this study. The procedures and the aims of this study were explained to the patients, and informed consent was obtained before their participation. All procedures were performed in accordance with the Declaration of Helsinki, and ethics committee approval was obtained from the local ethics commission (GO 14/106). Class I, II, III, IV, and V lesions on the permanent dentition were included in the study if they were clinically and radiographically diagnosed free from any pulpitis symptoms. Teeth with pulp exposure were excluded from the study.
Cavity preparation
Cavity preparations were performed by grade 4 (Group 1), grade 5 (Group 2), and postgraduate (Group 3) students. For cavity access, enamel walls were prepared using a high-speed hand piece with diamond burs under continuous water cooling. The superficial, soft, infected dentin was then excavated using sharp spoon excavators and round steel burs of different sizes, without water-cooling.
Visual-tactile assessment with and without magnifying glasses
Two experienced examiners (SG and FYC) assessed all cavities for residual caries using visual-tactile assessment. The examiners made a decision about the presence or absence of residual caries according to the hardness of the lesion area. The teeth were dried briefly using compressed air, isolated with cotton rolls and a saliva ejector, and viewed under standard dental lighting. The cavity preparation was considered as caries-free when a hard cavity floor was felt upon gentle pressure with a dental explorer14 that did not stick in the dentin. The presence of residual caries was recorded.
In the second step, the investigators used magnifying glasses (Keeler, Windsor, UK, ×3 magnification) to assess the cavities, and the recording process was repeated. Disagreements between the examiners were resolved through consensus.
FACE device assessment
Following the visual-tactile assessments, overhead fluorescent lighting was turned off and the light in the room was dimmed. Fluorescent violet light (405 nm, FaceLight, W&H Dentalwerk Bürmoos GmbH, Burmoos, Austria) was generated using a 100 - 130 watt xenon discharge lamp to evaluate caries removal. The operators inspected the cavity through a 500 nm red long-pass glass filter that was compatible with standard corrective goggles to visualize the orange-red fluorescing areas representing the bacteria-infected dentin surfaces (Figure 1). Green fluorescing areas and infected dentin tissue, which appeared dark brown or black, were recorded as caries-free.
Finally, all remaining carious areas that were diagnosed using these 3 methods were checked again and removed before the final restoration procedure.
Statistical analysis
Kappa statistics was used to evaluate inter-examiner and intra-examiner agreement regarding the clinical calibration for visual-tactile inspection with or without magnifying glasses and the FACE device. The data were analyzed using frequency analysis and the Chi-square test for independent groups. If the expected count in a cell was less than 5, the Fisher's Exact test was used. The McNemar test was used for the comparison of dependent groups (SPSS 20.0, IBM Corp., Armonk, NY, USA). The level of significance was set at α = 0.05. The relationship between the grade of the operators and the assessment methods was assessed. Furthermore, the obtained values for different diagnostic techniques were compared with each other.
Results
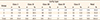
A total of 503 teeth (Class I, 105; Class II, 246; Class III, 101; Class IV, 17; Class V, 34 cavities) with carious lesions were prepared by students in grades 4 (Group 1) and 5 (Group 2), and postgraduate students (Group 3). The Chi-square statistical analysis revealed no significant relationship between the grade of students and the prepared cavity type (p > 0.05). Thus, the prevalence and variability of the prepared cavities were sufficient to perform statistical analyses. The distribution of the cavities is shown in Table 1.
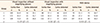
The inter-examiner reliability between the examiners was over 80%, showing excellent agreement between the examiners (kappa = 0.864). Caries were detected in 160 teeth examined by visual-tactile assessment without magnifying glasses, in 189 teeth by visual-tactile assessment with magnifying glasses, and in 234 teeth using the FACE device. The undergraduate students left higher numbers of cavities with undetected caries than postgraduate students for all assessment methods (Table 2). The relationships between grade and the presence of detected carious lesions using visual inspection with or without magnifying glasses were not found to be significant (p = 0.129 and p = 0.182, respectively). However, a significant relationship was found between grade and the presence of detected carious lesions using the FACE device (p = 0.018, Table 2).
Significant differences were found in visual-tactile assessments between Groups 1 and 3 (p < 0.001). The kappa values were substantial and mostly perfect (Table 3). A significant difference between inspection with the FACE device and visual-tactile inspection without magnifying glasses was found for Groups 1 and 2. The kappa values ranged from 0.463 to 0.761 (Table 4). A significant difference between inspection with the FACE device and visual-tactile inspection with magnifying glasses was found in Group 2. The FACE device detected more residual caries than visual-tactile inspection with magnifying glasses. The kappa values varied from moderate to substantial (Table 5).
Discussion
The null hypothesis was rejected, since the comparison of 2 caries-detecting techniques showed that the FACE device helped clinicians leave a cleaner dentin floor than the conventional visual-tactile method performed with or without using magnifying glasses. For the finalization of the caries excavation, visual-tactile assessment with or without magnifying glasses is still used by most clinicians. The problem is always to decide if the therapeutic endpoint has been reached and to distinguish between the dentin that should be removed and the dentin that can be safely left behind. In the ideal caries excavation technique, all carious tissue should be removed selectively, while leaving potentially remineralizable tissue on the cavity floor.13
Current caries excavation techniques are not considered sufficient to remove only the irreversibly destroyed carious tissue.115 Various methods and devices have been introduced for detecting residual caries, including caries detector dyes (CDDs), electronic caries monitors, and laser fluorescence light.1718 However, it has been reported that CDDs were not specific for infected dentin detection and mostly stained the dental-enamel junction or the circumpulpal dentin.19
Conflicting results have been reported for various fluorescence-based devices.3172021 Lennon et al.21 found that the FACE device was more effective in removing infected dentin than conventional excavation and excavation with the aid of CDDs. Lennon et al.22 also investigated the time required to excavate the infected dentin and reported a significantly shorter excavation time with FACE. Zhang et al.16 reported that the caries detection ability of the FACE technique was highly consistent and effective compared to laser-induced fluorescence, chemomechanical excavation, and conventional excavation.
The present study showed that use of the FACE device led to superior results in terms of detecting bacteria remaining in the dentin after excavation. Since more residual caries were detected using the FACE device, it can be asserted that the FACE device can provide a clinical aid in the detection of bacterially infected tissue. The only similar published data, in the study of Peskersoy et al.,23 also demonstrated that the FACE device led to a higher detectability than CDDs in the diagnosis and removal of carious dentin.
The present study also found that visual caries assessment performance was influenced by the use of magnifying glasses. More caries-free cavities were observed when magnifying glasses were used. This may have been due to the detailed visualization of the cavities provided by the magnifying glasses.242526 Zaugg et al.27 reported that dentists using magnifying glasses found more defects than their colleagues using no magnification tools at all. Studies conducted by Narula et al.,24 and Maggio et al.25 showed that magnification loupes significantly enhanced student performance in preclinical dental education and were considered an effective adjunct by the students who used them.
It should be noted that the present study has several limitations related to the FACE device and the study design. As the first step of the assessment process with the FACE device, which is based on light technology, the cavity should be fully opened and accessible. Therefore, unsupported but sound enamel may need to be sacrificed. The size of the light source also restricts the range of application of this technique.16 For example, it was more reliable for the examination of the cavity floor, rather than the cavity walls, due to the field of view. The FACE device works only on cavity locations that can be seen clearly. The lack of standardization of the cavity types and patient-related factors is a limitation related to the study design. Additionally, the caries excavation and examination procedures were more difficult in patients with limited mouth openings.




 XML Download
XML Download