

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
One of the key factors for the success of root canal therapy is accurate determination of the working length (WL).1 Various methods of determining WL include using radiographs, tactile sensation, and electronic apex locators (EALs). EALs for assessing the root canal length have gained popularity and eliminated many of the problems associated with radiographic measurements.2 Based on Suzuki's discovery that electrical resistances between the periodontal ligament and oral mucosa registered constant values of 6.5 kΩ, Sunada developed the first electronic apex locator in 1962.3 Whilst the simplest devices measure resistance, other devices measure impedance using high frequency, two frequencies, or multiple frequencies.4 The Root ZX (RZX, J. Morita Corp., Tokyo, Japan) is based on the ratio method for measuring canal length. This method simultaneously measures impedance values at 2 frequencies (8 and 0.4 kHz) and calculates a quotient of impedances. This quotient is expressed as a position of the file in the canal.5 SybronEndo Mini Apex Locator (MINI, SybronEndo, Sybron Dental, Glendora, CA, USA) is multifrequency based and is also claimed to be accurate in the presence of various intracanal conditions. Elements Diagnostic Unit and Apex Locator (ELE, SybronEndo, Sybron Dental) is a fourth generation apex locator which does not process the impedance information as a mathematical algorithm, but instead takes the resistance and capacitance measurements and compares them with a database to determine the distance to the apex of the root canal.6
EALs reported to be more accurate have evolved in recent years by improving the basic principles upon which the measurements are performed.7 Recently, a new multi-frequency technology based, pocket sized EAL Propex pixi (PIXI, Dentsply Maillefer, Ballaigues, Switzerland) has been introduced which uses multiple frequencies, in addition to calculating the root mean square (RMS) values of the electric signals but has not been extensively investigated.78
Numerous studies on apex locator have been performed, and generally they use only stainless-steel (SS) hand files for testing purposes. However, given the widespread use of nickel-titanium files, a comparison of the accuracy in determining length with an apex locator using stainlesssteel and nickel-titanium files (NiTi) seems clinically relevant.9 A literature search retrieved few articles comparing the accuracy of RZX using SS hand K-file and NiTi hand files but no published study was found that compares the accuracy of ELE, MINI and PIXI using SS hand K-file and NiTi hand files.910 Thus the purpose of this in vitro study was to investigate the accuracy of 4 EALs using SS hand files, and to compare the findings with NiTi hand files, respectively. The EALs tested were RZX, ELE, MINI, and PIXI. The null hypothesis was that there is no difference between canal length determination by SS and NiTi files by 4 EALs.
Materials and Methods
This study was approved by the Institutional ethical committee for research on human subjects or specimens (JSS/PGS/Ethical/2013-14/09). Sixty extracted, straight, single-rooted permanent human teeth with mature apices were selected for this study. Residual soft tissue on root surface was removed by soaking the teeth in 5% Sodium hypochlorite (Nice chemicals (P) Ltd., Kochi, India) for 3 hours. Teeth were stored in thymol solution until use. The type I canal configuration was confirmed by using digital radiograph (Gendex Oralix AC, Dentsply, Milano, Italy) in mesiodistal and labiolingual planes. Teeth with resorption, curvatures, open apices or radiographically invisible canals were excluded. The teeth were decoronated at the level of cementoenamel junction with a diamond disc to allow unrestricted access to the root canal and to provide a stable reference for all measurements. The coronal third of each canal was pre-flared using sequential Gates Glidden drills of sizes 4, 3, and 2 (Mani Inc., Tochigi, Japan), irrigated with saline, and pulp was extirpated with a barbed broach (Spiro Colorinox, Dentsply Maillefer).
Teeth were numbered 1 to 60 and the actual length (AL) was determined by introducing a size 10 or 15 K-file (Mani Inc.) into the canal until its tip reached a line tangential to the major apical foramen under a dental operating microscope (OPMI pico, Carl Zeiss, Oberkochen, Germany) at ×13.6 magnification. After carefully adjusting the silicone stopper to the reference point, the file was withdrawn from the root canal, and the distance between the file tip and silicone stopper was measured with a digital caliper (CD-6" CSX, Mitutoyo Corp., Kawasaki, Japan) to the nearest 0.25 mm. 0.5 mm was subtracted from this length and recorded as AL. To simulate the periodontium, this study used in vitro alginate model as described by Higa et al.11 Polystyrene specimen bottles (40 mL) were filled with alginate (Algitex, Dental Products of India, Mumbai, India). The apical two-third of the root was embedded in alginate and the lip electrode was also placed in alginate through another opening in the lid. Each EAL was used according to the manufacturers' instructions.811 The root canal was irrigated with 1% sodium hypochlorite (Nice chemicals (P) Ltd.) with a 23 guage needle, and depending on the size of the canal, a size 15 or 20 stainless steel hand K-file (Mani Inc.) was attached to the file holder and introduced apically into the canal until the EAL displayed '0.0' reading. The file was then gently retracted until the display showed stable '0.5' reading on the respective EAL. Two silicone stoppers on the file were adjusted to a coronal reference point, and the file was withdrawn to measure the distance between the silicone stopper and the file tip with a digital caliper. This was recorded as the electronically measured canal length (EL). The measurements were repeated with NiTi hand files (K-File NitiFlex, Dentsply Maillefer) for each EALs. To reduce variables, single calibrated operator experienced in the use of EALs carried out the electronic readings. Each file was used for ten measurements only and discarded. To ensure the humid condition of alginate model, all the measurements were recorded within 1 hour.
The results obtained (in mm) were tabulated. For both SS and NiTi hand files, differences between the AL and EL were calculated, and AL ± 0.5 mm was used to evaluate the accuracy of four EALs. Paired t test was used to statistically analyze the significance of mean differences between AL and EL. The percentage of clinically acceptable measurements recorded with EALs at ± 0.5 mm tolerance margin was analyzed with a chi-square test. Significance was set at p < 0.05. The analysis was performed with Statistical Package for the Social Sciences (SPSS 16.0, SPSS Inc., Chicago, IL, USA).
Results
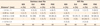
The mean differences between AL and EL measurements obtained with four EALs using SS and NiTi files are shown in Table 1. The incidence (%) of distance between AL and EL with SS and NiTi files are in Table 2.
With SS files, comparing the mean of AL with EL of four EALs, there was a statistical significant difference for RZX, MINI and PIXI (p < 0.05), and no significant difference was noted for ELE (p = 0.551). Similarly, with NiTi files, statistically significant difference was noted for MINI (p = 0.000), and no significant difference was noted for RZX, ELE, and PIXI (p > 0.05). There were statistically significant differences between SS and NiTi files for the mean difference between AL and EL for RZX and MINI (p < 0.05), and no significant differences for ELE and PIXI (p > 0.05, Table 1). The chi-square analysis found majority of readings (EL) with SS/NiTi file for each EALs within AL ± 0.5 mm range which was found to be significant (p = 0.000, Table 2).
Discussion
The goal of this in vitro study was to compare the accuracy of four EALs using SS and NiTi hand files. The main principle behind EALs is that human tissues have certain characteristics that can be modeled using a combination of electrical components. Therefore, by measuring the electrical properties (e.g. resistance, impedance) of that equivalent electric circuit, some clinical properties (such as the position of a file) can be extracted.4
The behaviors of EALs under various condition have been evaluated using a variety of laboratory models that mimic the electrical characteristics of human tissues.1112 Huang confirmed that physical properties influence root canal measurement and this formed the basis for in vitro models to test accuracy of EALs with various embedding media.612 In the present study, alginate was used for its various advantages like good electro-conductive properties, ease of preparation, stability, and firm consistency.11 Conducting solutions allow better electrical contact with the apical tissues and hence 1% sodium hypochlorite was used as an irrigant in the present study.13
It is generally accepted that the apical constriction (AC) is on an average located 0.5 - 1 mm short of apex.4 Kuttler found that the AC averaged 0.5 - 0.75 mm from the apical foramen and that the distance increased with age because of cementum deposition.14 However, there has been controversy as to whether EALs are able to determine the minor constriction or the major foramen.15 Diverse studies have usually considered the electronic measurements for the minor constriction to be between the 0.5 mm mark and the 1 mm mark.16171819 This in vitro study employed the '0.5' reading on the display/LED of all EALs as AC. To evaluate the accuracy of EALs, the ± 0.5 mm range from actual length was chosen, which is considered to be clinically acceptable and highly accurate guide.1520
Although many studies have investigated EALs, few have addressed the accuracy of EALs using NiTi files.9101115161718212223 NiTi alloy has been introduced for the manufacture of endodontic instrument since late 1980's.24 The NiTi alloys used in root canal treatment contain approximately 56 wt% nickel and 44 wt% titanium. In some NiTi alloys, a small percentage (< 2 wt%) of nickel can be substituted by cobalt.25 Compared with their stainless steel counterpart, NiTi files are much more flexible and are more resistant to torsional fracture providing the advantage during the preparation of curved root canals.26 Owing to the popularity of NiTi instruments in endodontics, Thomas et al. first investigated the effect of type of alloy (hand files) on the accuracy of EALs.9 Since then, various studies have been carried out using NiTi files (Rotary mode) with devices that integrate an electronic apex locator with an electric handpiece for canal preparation.102122 However, several potential limitations of the apex locator/motor combination such as risk of ledging, possibility of canal blockage, and the earthing of the endodontic motor may interfere with electrical circuit of the EAL.2122 Hence, the current study used hand NiTi files to evaluate the accuracy of the EALs.
The accuracy of RZX with SS file in present study was 93.3% which is in agreement with previously reported in vitro studies.1727 In vitro studies have shown the accuracy of RZX using SS files, varied from 76% to 100%.282930 The accuracy using the NiTi files was 70%. However, Siu et al. found this to be 50% using rotary NiTi instruments.10 Thomas et al. found both SS and NiTi files result in accurate readings with RZX and concluded these files could be used interchangeably.9 In the present study, there was a significant difference between reading with SS and NiTi files (p = 0.001). Thus the null hypothesis that there was no difference between canal length determination by SS and NiTi files was not supported for all EALs and was rejected.
The accuracy of ELE with SS file in the present study was 90% and was in good agreement with previous studies.1517 With NiTi files, the accuracy was 91.7% and there were no previous studies to corroborate the results. No significant difference were found between the readings with SS or NiTi files (p = 0.090). An accuracy of 95% was recorded in the present study for MINI with SS files which corroborates with a previous study, while the reported accuracy range from 77.7% to 100%.163031 Accuracy using NiTi files was 68.3%. However, Siu et al. recorded an accuracy of 39.29% using rotary NiTi files.10 In the present study, there was a significant difference between reading with SS and NiTi files (p = 0.000). The accuracy of PIXI with SS file in the present study was 83.3%. However, a previous study found this to be 88%.7 With NiTi files the accuracy was 83.3%. A literature search revealed no studies to corroborate the results of the current study. No significant difference was found between the readings with SS or NiTi files for PIXI (p = 0.351).
Sadeghi et al. evaluated Raypex 5 and found measurements (± 0.5 mm) with SS files and NiTi (Mtwo, nonrotary mode) to be 70% and 75% accurate, respectively.23 Neekoofar et al. evaluated Neosono ultima EZ and found SS and NiTi files to be 91% and 94% accurate, respectively.32 In present study, majority of the measurements for all EAL were within the ± 0.5 mm clinical acceptability with SS files. However, with NiTi files for RZX and MINI, this was only 70% and 68.3%, respectively. Although the reason for this is not completely understood, some studies have suggested the mechanism of MINI to be similar to RZX when subjected to various test conditions.2930 Thus, considering the lack of evidence supporting the reduced clinically acceptable range (± 0.5 mm from AL) of RZX and MINI with NiTi files, additional studies are warranted to investigate these EALs with regard to electrical properties of files used for measurements.
The variations in the accuracy of the EALs in current study may be attributed to the principle on which the EAL is based, operator sensitivity, experimental design, the electrical properties of the root canal walls, alloys and current conduction mechanisms in the canal. The electrical resistivity varied from 80 - 100 ohm-cm for NiTi alloy and 73 - 78 ohm-cm for stainless steel.2533 This slight difference in the electrical characteristic of the files may cause discrepancy in accuracy of EALs.21 However, to determine if this electrical characteristic of file type (alloy) had an effect on accuracy of EALs, clinical experiments similar to those conducted by Lee et al. needs to be undertaken.34 A detailed discussion about the electronic mechanism of various EALs is beyond the scope of this article. However, most of the previous studies have concluded that the type of alloy had no significant effect on accuracy of EALs.92332
It is important to note that the methodological decision to use the '0.5' reading on the display/LED of all EALs for all measurements could also have an effect on the accuracy of EALs in the present study, since studies have reported that '0.5' reading on EAL need not always be 0.5 mm short of the apical foramen nor does it indicate the position of apical constriction.3536
Although the present study used 1% sodium hypochlorite as an irrigant with all EALs, it is not clear if the electro-conductivity of this irrigant had any effect on the accuracy of EALs. According to Pilot and Pitts, with more conducting solutions, minimal changes in the electrical characteristics are noted as the foramen is approached and passed through. This minimal change would complicate electrical determination of foramen, because small changes may also occur as a result of other variable in the canal system.13 In a study, using two different generations of EALs under five different clinical situations, Venturi and Breschi revealed accuracy could be related to the contents of the canal. The study confirmed that the presence of nonconductive solutions inside the endodontic space achieves favorable effects on Apex Finder but negative effects on Root ZX.37
Root canals are surrounded by dentin and cementum that are insulators to electric current. At the minor apical foramen, however, there is a small hole in which conductive materials within the canal are electrically connected to the periodontal ligament that is a conductor of electric current.4 Meredith and Gulabivala found that the root canal acted as a complex electrical network with resistive and capacitive elements.38 It exhibited complex impedance characteristics having series of parallel resistive and capacitive components. They also suggested a complex relationship between the impedance of the smear layer and bulk dentin.38 Kim et al. analyzed electrical property measurement of EALs from ten papers in the literature, and they concluded that using the impedance ratio between electrical impedance measurements at different frequencies was a robust method for detection of the apical constriction.39 These phenomena surely influence the overall accuracy of all EALs, irrespective of their technical characteristics.38
The manufacturers of EALs should define the exact nature of their devices, how they operate electronically, and also should define the landmarks that their product is trying to locate (apical foramen versus minor foramen) which will help to understand and evaluate the effect of various newer files on the accuracy of newer EALs.16 The results obtained from this in vitro study cannot be applied to clinical situation because there is some inconsistency in EAL measurements even in fully controlled in vitro conditions. Recently, NiTi files (Controlled memory wire, M-Wire or R-Phase wire) with thermal treatment have been introduced to optimize the mechanical properties of these instruments.40 Future studies should focus on the effect of these NiTi instruments (Rotary mode) and their electrical properties on the accuracy of newer EALs integrated with handpieces.
Conclusions
Under the limitations of this in vitro study, it can be concluded that Root ZX was statistically more accurate with NiTi files compared to SS files, while MINI was statistically more accurate with SS files compared to NiTi files. ELE and PIXI were not affected by the alloy type of the file used to determine the working length.

 XML Download
XML Download