

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The main objective of root canal treatment is thorough shaping and cleaning of all pulp spaces and their complete obturation. A canal is often left untreated due to lack of meticulous diagnosis, and this untreated canal is one of the most common reasons for failure. Therefore, thorough knowledge on root canal configuration including characteristic features and anatomic variations is a key factor for successful root canal treatment.
One of the most important anatomic variations is the C-shaped root canal configuration. C-shaped root canal and its clinical implication was first described in dental journal in 1979.1 It has been difficult to diagnose and manage the C-shaped root canal because of its unique feature with presence of fins or webs connecting the individual root canals. This root canal configuration may occur in any molar area such as the mandibular first molar,23 first premolar,4 and maxillary molars.5 Above all, it is most frequently found in mandibular second molars.6 Owing to the high prevalence, the anatomic features of C-shaped root canal in the mandibular second molars have been well documented in many articles.678 The classification of them has been studied for decades, and the classification by Melton et al. and Fan et al. has been most representative criteria for typing C-shaped root canals.67 As the tooth anatomy varies according to the racial origin,910 the incidence of C-shaped root canals in mandibular second molars also has ethnic difference, which was higher in Asians than other racial groups.1112
Until now, there are only limited numbers of studies reporting C-shaped root canals in maxillary molars, and its classification has not been established. Considering the high failure rate of root canal treatment in maxillary molars, understanding the canal variation such as C-shaped root canal should be more emphasized. The aim of this study was to investigate the incidence of root fusion and C-shaped root canals in maxillary molars, and to classify the types by analyzing cone-beam computed tomography (CBCT) in a Korean population.
Materials and Methods
The research protocol of present study was approved by the Institutional Review Board of the Chosun University Dental Hospital (CDMDIRB-1218-90). For the analysis of root fusion and C-shaped root canals in maxillary molars, digitized CBCT images taken for orthodontic treatments at Chosun University Dental Hospital, Gwangju, Korea between February 2010 and July 2012 were examined. Among those CBCT data, the images of 911 subjects (393 male and 518 female) who had high quality radiographic data were selected for this study. Mean age of the patients was 21.9 years, ranging from 15 to 61 years. Fully erupted and completely root formed maxillary first and second molars without root canal treatment were included, and the third molars and immature teeth were excluded. Finally, total of 3,553 maxillary molars (1,786 first molars and 1,767 second molars) were examined retrospectively.
The CBCT images were taken with CB Mercuray (Hitachi medical Corp., Tokyo, Japan), while the scan settings were Φ 15 cm scan field of view, 0.3 mm voxel size, 120 kVp, 15 mA, with a 10 seconds exposure time. Tomography sections were displayed by PiViewSTAR and Rapidia MPR software (Infinitt Co., Seoul, Korea) in the axial, coronal, and sagittal planes. Contrast and brightness of images could be adjusted using the image processing tool of the software to ensure optimal visualization. The long axis of each tooth was determined and cross-sectional images at apical third were examined by rolling the tool bar from pulp chamber to the apex. The criteria for defining root fusion were adopted from Ross, which classified molars with fusion as fusion of entire root surface or one-third or less of the roots regardless of location of the fusion.13 As there are no criteria for defining C-shaped root canals, they were classified by the number of fused root, and subdivided by the root canal which constitutes the 'C' shape. In detail, if the C-shaped root canal was detected by the examiner, the number of roots was counted and then the involved canals in order were checked for naming it (e.g., Fusion of 2 roots, MB-P: C-shaped root canal made by 2 fused roots and the mesiobuccal root canal fused with palatal root canal).
The incidence of root fusion and C-shaped root canal between the first and the second molar was compared using Chi-square test. Statistical analysis was performed using SPSS (Version 18.0.0, SPSS Inc., Chicago, IL, USA) software. The differences were considered significant if the p value was less than 0.05.
Results
Classification of root fusion
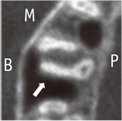
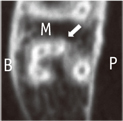
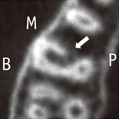
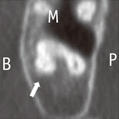
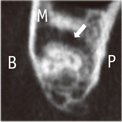
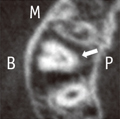
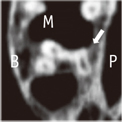
The type of root fusion was classified by the sequence of root which was fused. The roots and canals were briefly referred with abbreviation of capital letters, such as, B, buccal root/canal; MB, mesiobuccal root/canal; DB, distobuccal root/canal; P, palatal root/canal; MP, mesiopalatal root/canal; DP, distopalatal root/canal. The ' - ' between capital letters means fusion of roots or canals.
Total 9 types of root fusion are described in Table 1 and the representative CBCT images are presented. Generally, maxillary first and second molars have 3 roots. Therefore, the classification in the present study started with dividing fusion of 2 roots and fusion of 3 roots. There were also some teeth with 2 or 4 roots and those were classified into other types of root fusion. The difference between MB-DB-P and DB-MB-P was the sequence of fusion. The former made a C-shape with the opening to the mesial side, but the latter made a C-shape which opened to the distal side (Table 1). Teeth that have palatal root fused with mesiobuccal and distobuccal roots were divided into 2 types. In MB-P-DB (V-shape) type, fusion was done in serial manner and it looked like the letter 'V'. In 'All root' type, the cross-section image of coronal portion looked like the letter 'Y' or oval, and the cross-section image of the apical portion was circular (Table 1).
Incidence of root fusion in maxillary molars
Table 2 presented the type and number of root fusion in maxillary first and second molars. Root fusion was present in 402 (11.3%) maxillary molars out of 3,553 teeth examined in this study. The incidence of root fusion was higher in maxillary second molars (345 teeth, 19.5%) than in maxillary first molars (57 teeth, 3.2%).
Classification of C-shaped root canal
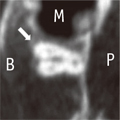
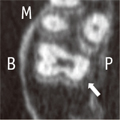
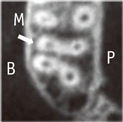
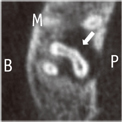
The type of C-shaped root canal was classified by each root canal which constitutes the 'C' shape. The abbreviations mean the same as used in root fusions. The fusion of root canals was classified into total 3 types according to the involved roots, and these types are also divided into subtypes. The classified types of C-shaped root canals are described with their representative CBCT images in Table 3.
From the representative images of each type of C-shaped root canal (Table 3), canals inside the roots may be separated even if the roots are fused. The C-shaped root canals could be formed by fusion of 2 roots (Type I) with the frequency of subtype C (MB-DB), subtype A (MB-P) and subtype B (DB-P) in a decreasing order. The two canals were fused partially or completely (Table 3). Larger C-shaped configuration was formed by fusion of 3 roots (Type II) with the similar frequency of subtype A (DB-MB-P) and subtype B (MB-P-DB) (Table 4). The three root canals were also fused partially or completely (Table 3). One tooth with 4 root canals was classified into Type III with the C-shaped root canal resulting from the fusion of MP with DP root canal observed in a maxillary second molar.
Incidence of C-shaped root canal in maxillary molars
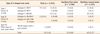
Table 4 shows the type and number of C-shaped root canals in maxillary first and second molars. Similar to root abbreviations, the capital letter represents each root canal instead of the root. C-shaped root canal configuration was present in 63 (1.8%) maxillary molars out of 3,553 teeth examined in this study. In first molars, the type of C-shaped root canal showed only Type I, subtype C (MB-DB: 15 teeth, 0.8%). In second molars, 48 teeth (2.7%) had C-shaped root canal and most common type was also Type I, subtype C (MB-DB: 29 teeth, 1.6%), followed by Type I, subtype A (MB-P: 11 teeth, 0.6%). The incidence of root fusion and C-shaped root canal was similar while their frequency in maxillary second molars was greater than that of maxillary first molars. Also, this difference was statistically significant (p < 0.001).
Discussion
This retrospective study investigated the incidence and type of root fusion and C-shaped root canals in the Korean maxillary molars using CBCT. Regarding the incidence of fusion in the maxillary first molars, our result (3.2%) was similar to those of Chinese (2.7%).14 Earlier studies in Burmese,15 Thai,16 Indian,17 and Chinese18 population reported no root fusion in maxillary first and second molars. Recent study in a Korean population reported 0.73% in the first molars.19 Other studies in the Caucasian,13 Chinese,20 and Irish population21 reported higher percentages of fusion in the first molars (7.7, 6.2, and 11.0%, respectively).
In the maxillary second molars, incidence of fusion (19.5%) was higher than the first molars, which is in accordance with the findings of several studies that reported higher prevalence in the second molar.1319202122
Earlier studies in Caucasian,13 Chinese,20 and Irish population21 reported higher percentages (52.9, 40.1, and 43.0%, respectively). A recent study in a Korean population reported lower prevalence (10.7%) than our result in the second molars.19 These differences among several studies could be caused by ethnic background, sample size, age of the subject, method of study, and criteria for defining root fusion. Our criteria for defining root fusion were adopted from Ross who classified the tooth with fusion of one-third or less of the roots as having fused root.13 However, the study reported lower incidence when a different criteria of regarding roots as fused only when fusion occurred on the entire root surface.19 It is still difficult to classify root numbers and shapes because there are no generally accepted guidelines.16 For example, in our study it was difficult to distinguish between MB root fused with DB root and one buccal root with 2 canals that joined at the apical part (Vertucci type II). General guidelines and clear definition of root fusion are necessary for comparing the results from other studies and for future studies.
In many studies, root fusion was classified into 5 groups.202122 But in this study, there were 9 types of root fusion because we separated fusion of all roots into 4 different types and presented two additional types. This classification provides more detailed information about morphology of maxillary molars. In our study, the most common type in the first molars was fusion of MB and DB roots. This result is consistent with previous reports.14202122 In the second molars, fusion of MB and P roots was the most common type in this study. This result is consistent with previous study in Chinese population,20 whereas other studies reported fusion of MB and DB roots as the most common type.2122
There were a few studies which reported C-shaped root canal configuration in maxillary molars. In 2002, De Moor reported estimated incidence of 0.091% in maxillary first molars by evaluating radiographs retrospectively.23 In a study from Chinese population using clearing method, Yang et al. reported 4.9% of incidence in the maxillary second molars.20 Our result was higher than that of the study of De Moor in the first molars, and lower than that of the study by Yang et al. in the second molars. These differences also could be due to ethnic background, sample size, age of the subject, method of study, and criteria for defining C-shaped root canal. In the study of Yang et al., classification was defined by connected orifice that resembles the letter 'C'.20
Several variations of C-shaped root canals in maxillary molars were also reported clinically.2324252627 Two earlier case reports described clinical cases of C-shaped root canal resulting from fusion of DB and P root canals.524 In our study, Type I, subtype B (DB-P) was similar to those cases. A previous study also reported 4 cases of C-shaped root canal resulting from fusion of DB and P roots (Type I, subtype B) in maxillary first molar.23 However, there were no Type I, subtype B (DB-P) in maxillary first molars in our study. Another previous study reported a case with Type I, subtype C (MB-DB).25 Two case reports using spiral CT or CBCT described that the C-shape resulted from merging of 2 palatal canals.2627 In our study, 3 types with 6 subtypes were found. Among these types, Type 2, subtype B (MB-P-DB) has not been reported earlier. Other 5 types correspond to the types described in previous reports. In agreement with previous reports, C-shape may also result from partial fusion of root canals, not only from the entire root canals.2627
The C-shaped root canal configuration in mandibular molars has typical root morphology and their classification has been well-documented and generally accepted.678 But in maxillary molars with C-shaped root canals, there is no common root morphology like mandibular second molar. And the C-shaped root canals are caused by different types of root fusion. Therefore, clear description and classification of C-shaped root canal configuration in maxillary molars are necessary.
Evaluation of root canal morphology employed many methods either in vivo or in vitro. The laboratory methods include canal staining and tooth clearing,1516202128 sectioning,611 in vitro radiography,10 in vitro macroscopic examination22 and micro-computed tomography.7 The techniques used in clinical studies include intraoral radiography,913 reviews of patient records,23 examination during endodontic treatment29 and CBCT.14171819 The advantages of computed tomography (CT) are noninvasive, and it allows 3D reconstruction and visualization of the external and internal anatomy. CBCT allows higher resolution, shorter scan time and reduction in radiation exposure than traditional CT scans.30 From the obtained personal data such as sex, age, and tooth position, inappropriate tooth samples could be excluded which might be included in the studies using extracted teeth ensuring the accuracy of the research.14 In our study, subjects had CBCT examination for orthodontic diagnosis and treatment, not for our study. So, additional cost, time and radiation exposure for this study were unnecessary. The large numbers of sample size can be easily obtained respectively because of digital imaging system. Despite these advantages, at present, CBCT has lower resolution than conventional radiographs.30 Thus, more accurate methods, such as clearing technique or micro-computed tomography using extracted teeth is inevitable to obtain more detailed information of root canal anatomy. Further studies using these techniques are needed for thorough information about C-shaped root canal configuration in maxillary molars and successful root canal treatment of this specific anatomic variation.
There were some limitations in this study. First of all, the CBCT data were concentrated in young patients (mean age: 21.9 years). This age distribution may be difficult to generalize the results into every Korean population. Because of their young age, there were numerous teeth with immature root apex and canals under formation. To overcome the misinterpretation of the results, we thoroughly exclude the immature teeth and teeth with improper image quality. We also used precise analyzing program for investigating the morphologies of roots and canals. In the future studies, wide range of patient age should be included in the study. Second limitation could be a calibration of CBCT image reading. To minimize the errors, we designed two independent reading systems which composed of two endodontists. When the results are inconsistent, the data was re-evaluated together and discussion was done for final reading. So the possible errors could be considered to minimum level.
Conclusions
This retrospective study of young Korean adults using CBCT data showed the incidence and types of root fusion and C-shaped root canals in maxillary molars. These anatomic variations were more frequent in the maxillary second molars. Two roots fusion (MB-P), and C-shaped canal with Type 1, subtype C (MB-DB) were the most dominant type. Although C-shaped root canals are most frequently seen in the mandibular second molar, they may also appear in maxillary molars. As the root canal morphology is one of the most significant factors for successful root canal treatment, the clinician should perceive these variations in maxillary molars.









 XML Download
XML Download