

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The primary goal of endodontic treatment is to debride and disinfect the root canal space to the greatest extent possible and then to seal the canals as effectively as possible.1 Therefore, understanding and recognizing the presence of unusual root and canal morphology is an essential prerequisite for the successful outcome of root canal treatment. Maxillary first molar is one of the most complex types of teeth by virtue of their multifaceted internal and external anatomy. Traditionally, the maxillary first molar has been described to have three roots, namely, the mesiobuccal, distobuccal, and palatal which form the 'tripod' or 'molar triangle', with three or four root canals, while the fourth canal commonly being found in the mesiobuccal root.2 There is a wide range of variation reported in the literature with respect to the number of roots and the number of canals in each root. Variations in root anatomy have ranged from 1 root to 5 distinct roots.3456 While as the canal variations have ranged from a single root canal to as many as eight root canals.37
When a maxillary first molar presents with an additional root, the teeth have represented three different morphotypes. The teeth may have an accessory palatal root, an accessory buccal root, or an accessory mesial root.8910 Table 1 summarizes various case reports of maxillary first molars presenting with more than three roots.56101112131415161718192021
In the dental literature, several terminologies have been interchangeably used to describe the two palatal roots. The two palatal roots are commonly referred to as mesiopalatal and distopalatal roots or mesiolingual and distolingual roots depending on their location on the tooth in situ. Carlsen and Alexandersen8 reported that when two palatal roots exist, one of them is the normal palatal root, while the other is a supernumerary structure. They coined the term radix mesiolingualis and/or radix distolingualis to refer to the extra palatal root.8 Another term used is first and second palatal roots.
Though the exact etiology behind this variation is still unclear, but its formation could probably be related to the splitting of the Hertwig's epithelial root sheath by exogenic or endogenic factors during the root development results in formation of two similar roots where it is difficult to differentiate which one is the accessory.22
The report describes the successful endodontic treatment of a unique case of a maxillary first molar with radix mesiolingualis and radix distolingualis, which has not been described earlier in dental literature. The identification of this anatomic aberration was done through clinical examination along with the aid of multiangled radiographs. Also a morphometric assessment of this morphology was made by the help of cone-beam computed tomography (CBCT) imaging.
Case Report
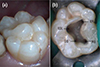
A 24 year old male patient with a non-contributory medical history was referred to the Department of Conservative Dentistry and Endodontics for root canal treatment in his right maxillary second premolar (tooth #15) and first molar (tooth #16). The patient gave a history of continuous pain for the past two weeks. The pain aggravated particularly on consuming anything hot or cold, on biting, or upon lying down. The patient had to take medication to get relief from pain. Clinical examination revealed a deep disto-occlusal and mesio-occlusal carious lesion on teeth #15 and #16, respectively. On the palatal surface of tooth #16, three well-developed lobulated cusps separated by a groove were also seen (Figure 1a). The preoperative radiograph revealed carious lesions closely approximating the pulp with widening of the periodontal ligament space with respect to teeth #15 and #16 (Figure 2a). In addition, two distinct root outlines of the palatal roots were observed with respect to tooth #16, suggesting an unusual anatomy (Figure 2a). Based on sensitivity tests and radiographic findings, a diagnosis of symptomatic irreversible pulpitis with symptomatic apical periodontitis with respect to teeth #15 and #16 were made. During investigations the patient informed that he had undergone CBCT investigation of the head for maxillofacial trauma. The availability of CBCT offered an additional opportunity to evaluate the tooth morphology of tooth #16. The patient was explained of the existing condition, and endodontic treatment was initiated.
The teeth were anesthetized, and the proximal surfaces of both the teeth were restored with posterior composite resin (P60, 3M ESPE Dental Products, St. Paul, MN, USA) to enable optimal isolation. Following rubber dam isolation, a conventional and a modified trapezoidal shaped endodontic access cavity were prepared on teeth #15 and #16, respectively, in order to gain access to both palatal canals. The coronal pulp tissues were removed with a spoon excavator, and the pulp chamber was flushed with 3% sodium hypochlorite solution (Cmident, Cmident, New Delhi, India). On inspection with a DG-16 endodontic explorer (Hu-Friedy, Chicago, IL, USA) under an operating microscope (Roslane Meditech, Haryana, India), the pulp chamber floor of tooth #16 revealed four canal openings corresponding to the two buccal and two palatal roots. The pulp chamber floor was quadrangular-shaped with four separate root canal orifices located in each corner. In addition, the mesial and distal orifices of the palatal roots were located more peripherally than those of the buccal roots (Figure 1b). Anticipating the presence of extra canals, further exploration of the pulpal floor was carried out for search of other orifices that were absent. The radicular pulp was extirpated using barbed broaches (Dentsply Tulsa, Tulsa, OK, USA). Endodontic treatment of tooth #15 was continued and completed in a single visit. As tooth #16 presented an unusual anatomy and images from advanced imaging were available, a more detailed assessment of the external and internal morphology of the molar was warranted before proceeding with the root canal treatment. Hence, tooth #16 was temporized with a sterile cotton pellet and Cavit G (3M ESPE Dental Products).
The data obtained was analyzed with the help of CS 3D imaging software (Carestream Dental LLC, Atlanta, GA, USA). CBCT images revealed that the three well-developed lobulated cusps were mere enamel overgrowth (Figure 3a). The images also confirmed that the tooth #16 had two buccal and two palatal roots each with distinct root canal and foramina at the apical level. The root trunk morphology was quadrangular with four emerging roots and four furcal entrances. The mesiopalatal and distopalatal roots were present relatively more mesial and distal to the chamber than where a single palatal root would exist (Figures 3b and 3f). Both the palatal roots were large, well-developed, straight, well-separated with bifurcation at the cervical level, and were more divergent and longer than the buccal roots (Figure 3f). The mesiopalatal root was longer than the distopalatal root (Figures 3f and 4a). The mesiopalatal and mesiobuccal roots were encaged in a web of root dentin up to the middle third. The distopalatal and distobuccal roots appeared to stand alone (Figures 3c - 3f).
At the next appointment, the patient was asymptomatic. Following rubber dam placement, temporary restoration was removed and canal patency was established in tooth # 16 with a size 10, 15, and 20 K-file. Working length was determined using an apex locator (Root ZX, J. Morita Corp., Tokyo, Japan) and was confirmed radiographically (Figure 2b). R25/0.08 and R40/0.06 single reciprocating files (Reciproc system, VDW GmbH, Munich, Germany) were selected for preparing the buccal and palatal canals, respectively. The files were set into motion with an X-Smart Plus contra angle 6:1 reduction handpiece (Dentsply Maillefer, Ballaigues, Switzerland) powered by a torque-limited electric motor (X-Smart Plus, Dentsply Maillefer). The files were used along with Glyde File Prep (Dentsply Maillefer) in a slow in-and-out pecking motion, ensuring that the amplitude of the in-and-out movements did exceed 3 - 4 mm. After every 3 complete pecking movements, the instrument was removed from the canal, and the canal was copiously irrigated with 3% sodium hypochlorite solution. After reaching approximately 2/3 of the canal length, working length was reassessed using an apex locator. Following which, the shaping and cleaning procedure was continued in a crown-down technique until the reciprocating file reached the working length. The canals were irrigated with 17% ethylenediaminetetraacetic acid (EDTA, Prevest Denpro Ltd., Jammu, India), followed by a final flush with sterile saline. Master cones (R25 and R40, VDW GmbH) were selected by placing cones corresponding to the Reciproc file used and was confirmed radiographically (Figure 2c). The canals were dried with absorbent points (R25 and R40, VDW GmbH) and obturation was performed using cold lateral compaction of gutta-percha and AH Plus resin sealer (Dentsply DeTrey, Konstanz, Germany). The access was then restored with a posterior composite resin. Final radiograph was taken to establish the quality of the obturation (Figure 2d). The patient remained asymptomatic at 2 months recall visit and was referred for permanent restoration with full-coverage porcelain crowns.
Discussion
In 2006, Cleghorn et al.23 did a comprehensive review of the root and root canal morphology of the maxillary first molar from the data obtained from various anatomical studies. One common finding in this extensive review was the absence of any study reporting the presence of one root or four roots, indicating that these variations to be very rare.23 However, more recent anatomical studies could establish the prevalence of two palatal roots in maxillary first molars. Neelakantan et al. investigated the root and canal morphology of 220 maxillary first molars in Indian population using CBCT, and found that two palatal roots have an incidence of 0.9% (2/220).24 Yang et al.25 investigated the prevalence of two palatal roots in maxillary molars in Chinese's population using CBCT. 528 patients comprising of 978 maxillary first molars were studied, and they concluded that the prevalence of two palatal roots is as low as 0.31% (3/978).25 Rouhani et al.26 evaluated the external morphology of the roots and analyzed the root canal configuration of maxillary molars in Iranian population by means of CBCT technique. Out of the 125 maxillary first molars evaluated, two molars had four roots (1.6%); one with fusion of the mesiobuccal and mesiopalatal roots and the other with fusion of distobuccal and distopalatal.26 Gu et al.27 investigated the incidence and anatomic features of 4 rooted permanent maxillary molars in a North Western Chinese population using CBCT. Out of 719 patients comprising of 1,365 maxillary first molars, they found only one tooth had two palatal roots (0.07%).27 Georgia et al. evaluated the root and canal morphology of maxillary permanent molars using CBCT in Greek population and found that out of the 410 first molars examined, one tooth had an accessory mesial root, and four teeth had two palatal roots (0.97%).28 Tian et al.29 analyzed and characterized the root and canal morphologies of maxillary molars in 844 Chinese patients using reconstructed CBCT imaging. Out of 1,558 maxillary first molars studied, they found 1 tooth with four separate roots (0.06%).29 No literature could be found in which double palatal roots could be considered a racial characteristic. However, photographs and radiographs of some Australopithecus maxilla seem to show this trait with double palatal roots centered over large distopalatal and mesiopalatal cusps.19
Although the incidence of four-rooted maxillary first molars with two palatal roots is rare, they do occur.61112131415161718192021 Diamond was the first to illustrate in his textbook examples of two extracted maxillary first molars with two distinct and widely divergent palatal roots.30 Christie et al.19 during their 40 years of clinical practice found 16 cases of maxillary molars (14 were second molars, and only 2 were first molars) with two palatal roots. They stated that of all variations seen in maxillary molars, the least frequent anomaly appears to be that of the double palatal root. In an effort to classify root morphology of maxillary molars with two palatal roots, they evaluated the radiographs of 16 endodontically treated molars and the slides of six extracted teeth. They identified three radicular configurations based upon the shape and degree of separation of the palatal roots (Table 2).19 Baratto-Filho et al. in an anatomical study on two extracted maxillary second molars with two palatal roots found one molar to be of a different morphology from that described by Christe et al. and suggested to include this variety in the classification as Type IV (Table 2).1819
Versiani et al. stated that Christe's classification was not feasible considering that fusion of roots might occur in different levels. They examined the anatomy of 25 extracted permanent 4 rooted maxillary second molars in a Brazilian population using micro-computed tomography and proposed a new classification based only on the divergence of the roots. They combined Christe's Types II and III into one category (Type II) and a new variation was described as Type III (Table 3).1931
Carlsen and Alexandersen8 proposed another classification based upon their observation of a collection of 145 extracted permanent maxillary molars with root complexes having two palatal roots at the School of Dentistry in Copenhagen. Three different variants were identified based upon the affinity of the roots to the very pronounced, mesiopalatal or distopalatal or mesiopalatal and distopalatal aspect of the crown. They were classified as separate, non-separate, and separate/non-separate depending upon their association with mesiobuccal, distobuccal, and lingual root component of these teeth (Table 4).8
Carlsen and Alexandersen8 in their study found 81 radix mesiolingualis, 7 radix distolingualis, and 57 radix mesiolingualis/distolingualis. Nine teeth were maxillary first molars, of which 7 were identified as radix mesiolingualis, 2 were radix mesiolingualis/distolingualis but no radix distolingualis was found. Out of the 7 radix mesiolingualis, 4 were separate, 2 were non-separate, and 1 was separate/non-separate type. While as, both the radix mesiolingualis/distolingualis were separate.8 The tooth described in this report is a case of radix mesiolingualis/distolingualis separate/non-separate type according to Carlsen and Alexandersen classification and Type I according to Christie et al. and Versiani et al. classification (Figures 1, 2a, and 3).81931
Of the various cases of maxillary first molars with two palatal roots reported, it was interesting to note that the majority of cases presented a Christie et al.19 Type I pattern.101415182021 It is important to note that except Type I, identifications of other variants are very difficult on a radiograph alone but are more obvious when extracted teeth are examined. Based on the same observation, Christie et al. grouped Type II and Type III molars together.19 However, in clinical situations use of computed tomographic imaging would be beneficial.
In regard to the internal canal morphology, the most common canal configuration seen is individual palatal roots with separate root canal and foramina at the apical level.6101314151718192021 Variations reported include distopalatal root with one root canal, which divides into two and then merges to exit through a single apical foramen (1-2-1), and C-shaped palatal root canal with a palatal root bifurcation at the junction of the middle and apical third.812 An interesting observation seen in the case reports of maxillary first molar with two palatal roots is the presence of a single canal in the mesiobuccal and distobuccal roots.61112131518192021
It has been shown that the rarer the aberration, the more likely it is to be bilateral in occurrence.32 While, bilateral occurrence of maxillary first molar with two palatal roots has been reported.17 Asymmetric morphology has also been reported in which one side showed a maxillary first molar with two palatal roots while the contralateral tooth had either two palatal root canals in a single palatal root, or one palatal root canal in a single palatal root.1319 Yang et al. in their study reported that the prevalence of two palatal roots was neither affected by patient's gender (female vs. male) nor by topology (right vs. left side).25 In our case, the contralateral tooth had a normal anatomy with one palatal root and a single palatal canal (Figure 3).
Diagnosis of maxillary molar with extra palatal root is challenging. Clinically, the presence of periodontal pockets and/or gingival recession can facilitate the identification of the external root anatomy, such as palatal root bifurcation.6 Sometimes the presence of palatogingival groove on the lingual surface of the crown and root may indicate the presence of two palatal roots because this may represent an abortive attempt to form two palatal roots.33 There has been report of concurrent existence of enamel pearls (cervical enamel projections) in the furcation area of maxillary molars with two palatal roots.81931 Carlsen and Alexandersen in their study observed that almost 70% of maxillary molars with two lingual root structures were associated with voluminous enamel extension between them. They reported that enamel extension of this nature only appears on maxillary molars with two lingual root structures and should be considered as a marker variable for this root constellation.8
Another landmark suggestive of the presence of an extra palatal root is the presence of an additional cusp or cusps on the buccal or lingual surface of the molar crown, making the crown appear relatively larger than the normal.8 It is important to note that an increased number of cusps is not necessarily related to an increased number of roots. However, an additional root is nearly always associated with an increased number of cusps and with an increased number of root canals.34 In addition, a very pronounced, mesiopalatal or distopalatal or mesiopalatal and distopalatal aspect of the molar crown is seen to be associated with extra palatal root.8 A similar observation was made in the case reported here. Occurrence of a prominent cusp, such as the one reported by Thews et al. wherein the distolingual cusp was absent in the maxillary first molar and a single, enlarged cusp occupied the entire lingual half of the crown was reported to be associated with extra palatal root.21
Radiographs play an important role in detecting such anatomic variations. When examining the preoperative periapical radiographs of maxillary molars, if the outlines of the roots are unclear, the root canal shows sharp density changes or the apices cannot be well defined, then extra roots can be suspected.35 When a straight-on periapical radiograph is being assessed, and the palatal root cannot be identified between the mesiobuccal and distobuccal roots; the existence of two palatal roots should be suspected.36 When the palatal roots are in the same buccolingual plane with that of the buccal roots, taking additional radiographs from a 20 degree mesial or distal angulation will aid in revealing the periodontal ligament outlines and facilitates detection of extra palatal root. In our case, a straight-on periapical radiograph of the maxillary right first molars revealed the outline of the periodontal ligament space of the two buccal and two palatal roots as the palatal roots were longer and divergent compared to the buccal roots (Figure 2a). The confirmation was done by CBCT investigations (Figure 3).
A more definite means of determining the presence two palatal roots is by visualizing the pattern of the pulp chamber floor. When two palatal roots are present and are widely divergent (Type I), the pulp chamber floor takes quadrangular-shape with one canal orifice located in each corner. The mesial and distal orifices of the palatal roots will be present more peripherally than to those of the buccal roots (Figure 1b). But when the palatal roots run parallel (Type II), the orifices of the palatal roots are usually located along the same horizontal line as that of the buccal roots, with the pulp chamber floor taking a square, rectangular or a rhomboidal shape.
Yang et al.25 reported that the mean interorifice distance between the palatal canals was 2.84 ± 0.50 mm, while that between the buccal canals was 2.15 ± 0.82 mm. They also found that the average angle among the palatal roots was significantly larger (34.6 ± 16.1°) than between the buccal roots (21.3 ± 12.2°).25 In the case reported here, the interorifice distance between the palatal canals was 5.12 mm and that between the buccal canals was 2.66 mm (Figures 4b and 4c). Both the mesiopalatal and distopalatal angles were acute (Figures 4d and 4e). The palatal roots revealed a divergence of as much as 41.2° between them (Figure 4a). When a maxillary molar demonstrates palatal root bifurcation in the apical third, the bifurcation can be identified by the eccentric position of the file inside the palatal root canal, either clinically during exploration of the canals or radiographically during working length determination.36
The most valuable tool to identify and evaluate the morphological features of the two palatal roots is by CBCT imaging. CBCT allows the creation of images not only in the axial, coronal, and sagittal planes, but also in oblique or curved planes. CBCT data are also amenable to reformation in a volume, allowing three-dimensional reconstruction of root and canal system. They eliminate the problem of superimposition of roots with surrounding anatomical structures such as the zygomatic arch and the floor of the maxillary sinus seen on conventional radiographs, which makes detection of additional palatal root difficult. In the present case, availability of CBCT scan images not only helped in confirming the presence of two palatal roots, but morphometric analysis of the tooth provided important information of the crown and root anatomy.
Presence of an extra palatal root is of significant importance while planning endodontic treatment. Foremost, the identification of this additional root avoids missing a canal, which could lead to complications and treatment failure. A modification in the access cavity design is usually a common landmark for teeth having an accessory palatal root, especially when they are well separated with a coronal bifurcation. Teeth with divergent palatal roots (Type I) often have a pulp chamber with wider mesiodistal dimensions over the palatal cusps. The palatal wall of the access cavity needs to be extended more in a mesiodistal direction to locate and gain access to the well separated canal orifices (Figure 1b). Hence, it is important that the conventional triangular access cavity outline be modified to a trapezoidal or rhomboidal form which reflects the shape of the pulp chamber of these teeth. When the palatal roots run parallel (Type II) and are closely related to each other, the access cavity outline will take on a square or rectangular or a rhomboidal shape, rather than the triangular form. However, when the palatal root demonstrates bifurcation in the apical third, the access cavity configuration may not need to be changed significantly.
Before beginning with the mechanical instrumentation of the root canal, it is important that root and canal morphology of the palatal roots are assessed to prevent the incidence of shaping aberrations. In three rooted maxillary first molar, the palatal root is more broad mesiodistally than buccolingually and ovoid in shape. The palatal canal is ovoid mesiodistally and as it tapers toward the apex, it becomes small and round. In the present case, the distolingual root was round and conical in shape with depressed-round to an almost-round canal along the entire root length. While as, the mesiopalatal root was broad buccolingually than mesiodistally. The mesiopalatal canal was ovoid in buccolingual direction and toward the apex, it became round. On the distal aspect of the mesiopalatal root, a concavity was observed, resulting in a wall with less dentinal thickness (Figures 3a - 3c). As this zone is prone to strip perforation, mesiopalatal canal orifice was relocated more mesially (away from furcation), and care was exercised not to instrument this wall excessively.
Carlsen and Alexandersen8 reported that the palatal roots often presented a sharp apical bend of around 90°, especially in teeth where the root structures were separate. The direction of the bend often varied. The clinician must be aware that when the palatal roots curve buccally at the apical one third, the curvature will not be apparent on a standard periapical radiograph. Failure to recognize such a curve may lead to perforation of the root during cleaning and shaping procedure. Hence, following relocation and enlargement of the canal orifice, initial exploration of the root canal must be done with small-sized stainless steel K-files as they often give the impression of the canal, thereby guiding the clinician to the curvatures presented in the canal.8
Carlsen and Alexandersen also observed that the palatal roots frequently appeared with apical slenderness, especially when the root structures were separate. The degree of slenderness was occasionally extremely pronounced.8 Therefore, during cleaning and shaping NiTi instruments of suitable size and taper must be used with caution to avoid stripping or perforation caused by over-enlargement of the relatively thin root canals.
Conclusions
The prognosis of maxillary first molars with additional palatal root that require root canal treatment should be considered the same as that of any other first molar as long as all the root canals are located and adequately treated. A thorough knowledge of all the diversities, careful interpretation of angled radiographs, proper access preparation and a detailed exploration of the pulp chamber floor under magnification is paramount for identification and successful endodontic management of teeth with such anatomic aberrations.






 XML Download
XML Download