

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Vertical root fractures (VRFs) have been defined as a single longitudinal fracture beginning either on the apical or coronal aspects of the root of a tooth.1 These fractures may originate anywhere on or within the root and may extend coronally toward the cervical margin in the facial or lingual aspects. When the tooth segments are separable, the fracture is termed complete, as it involves two root surfaces; otherwise, the fracture is incomplete and involves one root surface.1 VRFs can occur as the result of external trauma, chewing forces, or occlusal trauma to the involved tooth, and can evolve over time both longitudinally and horizontally.1 Their prevalence is higher in endodontically treated teeth and in the presence of posts, most likely due to over-preparation of the root canal during endodontic treatment.2 If VRFs evolve over time to split the tooth root, the prognosis of the tooth may be adverse, requiring extraction and replacement.3 Due to the rapid development of VRFs and the difficulty of managing advanced VRFs, the early diagnosis of such lesions is fundamental for preserving the affected tooth.4 The diagnosis of VRFs can be extremely challenging due to the lack of pathognomonic signs and symptoms, as well as the lack of accurate radiographic instruments for identifying such fractures.4 Although some radiographic features (such as the so-called halo appearance) can be found frequently in the presence of a VRF, most of these radiographic patterns are easily confounded with a combined bacterial endodontic-periodontal lesion.56 Moreover, three recent systematic literature reviews have found that VRFs cannot always be considered detectable even with the aid of cone-beam computed tomography (CBCT), most likely due to the small size of the lesions, which can be smaller than the voxel size.789 Often, the diagnosis of VRF is facilitated by indirect signs, such as the detection of a single narrow periodontal defect, the presence of a sinus tract, usually located in the region of the middle portion of the root, and mild pain during chewing or after percussion.4 When the diagnosis is doubtful, it may be necessary to perform an exploratory flap.1011
Although the prognosis of vertically fractured teeth is often poor, requiring tooth extraction,12 conservative approaches have also been described, either through the use of bonding fragments and reimplantation13 or through surgical treatment.11 The reparative treatment of VRF is significantly different from the bonding approach. Taschieri et al. published the results of a case series investigating the results of surgical abrasion of the fractured portion of the tooth through the use of burs and further filling of the cavity with mineral trioxide aggregate (MTA).11 In their approach, the space was managed as a cavity created during endodontic surgery. This particular technique may provide good outcomes in cases of incomplete fractures and in cases requiring complete removal of the fractured portion, potentially removing all bacterial infiltration.
The aim of this report was to present the case of a patient requiring reparative surgery for the treatment of an incomplete VRF affecting a traumatized tooth.
Case Report
A 26 year old male reporting vague signs and symptoms localized in the region of the maxillary left central incisor (Tooth #21) was referred to the Department of Dentistry at IRCCS Istituto Ortopedico Galeazzi in Milan, Italy for an endodontic specialist consultation. The patient reported that a traumatic injury to that region had occurred three years before the visit. Dental anamnesis revealed a previous orthograde treatment performed shortly after the previously mentioned injury, based on the diagnosis of pulp necrosis. Endodontic surgery was then performed eight months later. The patient stated that the endodontic operation was a consequence of the persistence of a radiographically detected periapical lesion and the presence of vague but bothersome signs and symptoms.
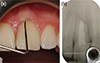
A clinical examination showed a moderate swelling on the vestibular side in the region of tooth #21, as well as the presence of a sinus tract in the same area, approximately 4 mm from the gingival margin (Figure 1). A narrow periodontal defect 7 mm in depth was present on the buccal side, as evaluated using a periodontal probe. A radiographic examination performed before surgery using both periapical radiographs and CBCT (J. Morita MFG Corp., Kyoto, Japan) revealed a root-end resection, a periapical radiolucency, and a widening of the periodontal ligament space at the mesial aspect of the root, although no hair-like fracture line radiolucency was noted in the tooth, except in the CBCT horizontal projection that showed an incomplete VRF 3 mm from the apex (Figure 2).
The diagnostic hypothesis was of a VRF. This lesion can mimic other diseases (periodontal and/or endodontic) both clinically and radiologically.56 These features can lead to difficulties in diagnosis. A patient's dental history together with clinical and radiographic findings serve as the basis of a diagnostic hypothesis that requires further confirmation in order to determine the prognosis and treatment of each clinical case. As stated before, in many cases, an exploratory flap is necessary to make a correct diagnosis.10
Preoperatively, the patient was fully informed about the surgical protocol and personally signed and dated the consent form before the intervention. The patient rinsed his mouth with an antiseptic mouthwash containing 0.2% chlorhexidine digluconate to reduce the risk of contamination of the surgical field. The access flap was triangular, with one horizontal incision and one vertical incision, with the latter located distally to tooth #23. A papilla base incision (PBI) approach was adopted, as described by Velvart and colleagues.1415 Magnifying surgical loupes (×4.3) were used for enhanced visualization of the flap design and management. The flap was irrigated continuously to prevent dehydration of the periosteum.
Following flap elevation, evidence of buccal bone fenestration was clearly detected (Figure 3). The granulation tissue was removed until the anatomical structures of the exposed root portion and the alveolar bone margins were clearly visible. After exposure of the root, the type of the fracture was determined using the microscope as a magnification device. In order to detect the extent of the fracture, 1% methylene blue dye was used as a marker (Figure 4).
A VRF involving the apical and partially the medial portion of the root was identified. The root end was removed by abrasion using a fissure bur at the desired angle (approximately 25°, in order to ensure direct visualization), removing more than two-thirds of the fracture line. A root-end cavity was prepared using a zirconium nitrate retro-tip (Dentsply Maillefer, Ballaigues, Switzerland) driven by an ultrasonic device unit (Piezon Master 700, EMS, Nyon, Switzerland, Figure 5).
The remaining part of the fracture line (approximately 2 mm) was treated using the abovementioned retro-tip, and a groove was made following the remaining fracture line. In this way, an L-shaped cavity was created. The morphological integrity of the intracanal structure was carefully checked using a microscope (Carl Zeiss, Oberkochen, Germany) in order to avoid the possibility of fracture propagation on the other sides of the root.
When the root-end cavity was created, the ultrasonic device unit was set at no more than half power under constant and copious sterile water irrigation. The cavity was then dried using a paper cone and examined again in order to detect root-face alterations. Finally, MTA (ProRoot MTA, DENTSPLY Tulsa Dental, Tulsa, OK, USA) was used as the root-end filling material (Figure 5). A curette and gauze was used to remove the excess filling material. Platelet-rich plasma (PRP) and a resorbable membrane was used to cover the bone defect. The PRP was prepared following the instructions provided by the manufacturer (PRGF System, BTI Biotechnology Institute, Vitoria-gasteis, Alava, Spain). A few minutes before it was used, 50 µL of 10% calcium chloride (CaCl2) per millilitre of plasma rich in growth factors was added to enable clot formation. This resulted in a gel with fair mechanical consistency that was stable and easy to handle.
In order to mobilize the flap and facilitate its repositioning, periosteal incisions were performed, releasing muscle tension. The reflected tissues were then replaced into their original position and sutured with a non-resorbable 5-0 suture (Ethicon Inc., Piscataway, NJ, USA, Figure 6).
After surgery, the patient was advised to avoid mouth rinsing, hard and hot food, hot drinks, heavy physical work, and tooth brushing on the day of surgery. The patient was instructed to rinse his mouth twice daily with 0.2% chlorhexidine digluconate for plaque control up to 10 days after surgery. Non-steroidal analgesics (ketoprofen) were prescribed after the surgical procedure for pain relief and/or swelling control if needed. Sutures were removed five days after surgery.
Discussion
The present case report discusses the treatment of a tooth affected by a periradicular lesion of infectious origin that followed the occurrence of a VRF in a maxillary central incisor. This approach to the surgical treatment of the lesion, even though it required adequate expertise to be effective, may be expected to allow tooth retention, given the absence of any signs or symptoms of infection or periradicular inflammation observed in follow-up visits.
The treatment protocol presented in this report was derived from the protocol described in a 2010 study published by Taschieri et al.11 In that case series, subjects who presented with an incomplete VRF located in the coronal portion of the tooth underwent surgical treatment after removal of the fracture itself, followed by sealing of the space thereby created with MTA. Five years after the treatment, two of the seven treated teeth were considered to be failures and removed. Since the only alternative to such a surgical approach is tooth extraction and subsequent replacement, the results of that study can be considered encouraging.
Another issue that must be considered is the timing of the treatment. It is known that VRFs can evolve over time, extending apically or coronally and involving the other side of the affected root, thereby limiting the possibility of surgical treatment to a significant extent.116 Unfortunately, the extent of the VRF can be appropriately diagnosed only through direct observation after the creation of an exploratory flap with the aid of magnification devices and/or staining dyes. In cases with an adverse prognosis, the possibility of placing an implant immediately after tooth extraction, in a single visit, has also been discussed.3 Since the VRF can evolve over time, the bone defect associated with the fracture may also change over time. As described in the literature, the causes of apico-marginal bone dehiscence are related to bacterial migration from the inner space of the tooth, through the fracture, to the periodontal ligament space.17 Here, the bacteria can initiate an inflammatory reaction in the connective tissue, resulting in bone resorption and formation of a periodontal pocket, which may also become populated by periodontal pathogens.1819
In this particular case, the clinical absence of signs and symptoms and the radiographic findings indicating the ongoing resolution of the periradicular radiolucency could be interpreted as the consequence of removal of the communication between the periodontal ligament space and the tooth canal space. Previous studies have reported that periapical re-surgery, even though challenging, may be feasible in cases of recurrence of an endodontic lesion.2021 In this case report, endodontic re-surgery was performed, removing the infected root end without any clinical or radiological signs or symptoms of recurrent periapical infection.
Platelet concentrates have been described in the literature as being able to significantly reduce the impact of endodontic surgery on postoperative quality of life,22 as well as in cases of accidental perforation of the maxillary sinus membrane.23 Moreover, they have been observed in both in vitro and in vivo studies to enhance soft tissue healing24 and to reduce the risk of postoperative infection due to their potential antimicrobial properties.2526 In this particular case, the PRP was applied to cover the defect and was in contact with the soft tissue that was reflected and then sutured.
Conclusions
In conclusion, the present case report showed that a surgical approach may be effective for treating a combined endodontic-periodontal lesion originating from an incomplete VRF and a recurrent periapical lesion. The treatment involves removing the fracture and the root end, followed by sealing the resultant cavity in order to avoid bacterial migration. Randomized controlled clinical trials on a large sample of patients would be helpful in understanding the clinical efficacy of the treatment protocol described in the present report.







 XML Download
XML Download