

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Dental caries can be distracting and painful and, if neglected, can cause serious problems elsewhere in the body.1 The pain of caries can reduce a person's working efficiency, which in turn affects the economy. Dental caries affects humans of all ages in all regions of the world and is the most prevalent chronic disease in humans. According to the World Health Organization, three quarters of the world's population suffers from dental caries. Worldwide, 60 - 90% of school children and nearly 100% of adults have dental caries.23 Dental caries remains a public health problem, particularly among the underprivileged groups in developed and developing countries without access to treatment care.4
Extensive research in the field of modern dentistry has led to the development of various restorative materials and different modalities for the treatment of dental caries, mainly tooth restoration in the early stages.56 However, 70% of restorations need to be replaced due to the formation of secondary caries.6 The risk factors for secondary caries are identical to those for primary caries. Unfortunately, it is not possible to accurately predict which patients are at risk of restoration failure.7 The existing literature describes three therapies to guarantee against a continuous caries process or the reactivation of residual caries: restriction of the nutrient supply by isolating the caries process from the oral cavity, operative treatment, that is, excavating the carious dentin, and the use of a cariostatic filling material.8 The last measure is one of the most studied with respect to the concept of minimally operative intervention.
During the last few years, a variety of dental restorative materials have captured the market.9 Among them, glass ionomer cements (GICs) possesses certain unique properties that make them useful as restorative and adhesive materials, including adhesion to the tooth structure and base metals, anticariogenic properties due to fluoride release, thermal compatibility with the tooth enamel, and biocompatibility. The antibacterial activity of GICs may be attributed to the low pH of the cements before setting and/or their fluoride release. Recently, there have been considerable changes in the formulations and handling properties of the GICs for different clinical applications.10
Of the various brands available in the market, Fuji IX and Ketac Molar have shown good antimicrobial properties. One of the recently introduced cements, d-tech has been more popular in private dental clinics and dental educational institutes because of its low cost as compared to that of Fuji IX and Ketac Molar. Further, d-tech GIC is a humid-stable restorative cement with fluoride releasing properties. Newer materials need to be tested in an attempt to decrease the rate of treatment failures. Studies investigating the antimicrobial efficacy of these newer materials need to be carried out to reduce the frequency and the severity of secondary caries.
Microorganisms play an important role in the initiation and progress of dental caries. Streptococcus mutans (S. mutans) is the primary bacterium responsible for caries initiation and Lactobacillus acidophilus (L. acidophilus) is the principal bacteria related to caries progression and is responsible for the formation of secondary caries. Hence, in the present study, we evaluated the antimicrobial activity of these restorative GICs on S. mutans and L. acidophilus. The null hypothesis states that there is no difference in the antimicrobial effect of three different restorative GICs on S. mutans and L. acidophilus.
Material and Methods
The present study was an in vitro experimental study done in order to assess and compare the antimicrobial efficacy of three different GICs on S. mutans (ATCC-25175) and L. acidophilus (ATCC-4356). The cements used were Fuji IX (GC India Dental Private Ltd., Telangana, India), Ketac Molar (3M Co., 3M India Ltd., Bangalore, India), and d-tech (Sakhi Chem Tech (I) Pvt. Ltd., Pune, India).
Ethical clearance was obtained from the Institutional Review Board (MUHS/PG-T/E-2/868/2012) of ACPM Dental College and Hospital, Dhule, Maharashtra State, India. The study was carried out in a private microbiology laboratory. The antibacterial effect of each GIC was evaluated against S. mutans and L. acidophilus by using an agar plate diffusion test. A pilot study was conducted to check the feasibility of the procedure and to assist in the determination of the sample size for the main study. On the basis of the data obtained from the pilot study, that is, the mean zone of inhibition for each group and the effect size, the sample size needed for each group was calculated using G*power software,11 and was found to be 15 plates per group.
Preparation of bacterial culture and agar plates
Microbial analysis was performed in a private research laboratory. Each of the indicator strains collected from Hi Media Laboratories, Mumbai, Maharashtra, India, was grown in 15 mL of brain-heart infusion (BHI) broth, separately for 48 hours at 37℃ according to the physiological characteristics of each microorganism. The resultant bacteria were again placed in 5 mL of the BHI broth for 24 hours at 37℃ to form a suspension (inoculum), corresponding to 106 CFU/mL using the McFarland scale.12 In each sterilized petri dish (height, 15 mm; diameter, 150 mm), a base layer containing 15 mL of BHI agar was prepared. Thirty plates were prepared and divided into two groups, namely Groups I and II, with each group containing 15 petri dishes. The larger end of a cooled, flamed pasteur pipette was used for making three wells (diameter, 4 mm) in the agar plates.
Mixing and placement of cements
GICs were mixed according to the manufacturers' instructions (1 level scoop of powder to 1 drop of liquid for both Fuji IX and Ketac Molar, and 1 level scoop of powder to 2 drops of liquid for d-tech). Standard amounts of powder and liquid were dispensed onto the mixing pad. By using an agate spatula, we divided the powder into two parts. The first part of the powder was incorporated into the liquid and spatulated for 10 seconds and later, the remaining portion of the powder was incorporated and mixed thoroughly for 10 - 15 seconds. The wells were completely filled with Fuji IX, Ketac Molar, and d-tech cements, respectively. The microbiologist was blind to the coding of the plates. A Teflon-coated instrument was used for condensing the GIC into the wells. Petri dishes in Groups I and II were inoculated with S. mutans and L. acidophilus, respectively. Each petri dish was inoculated with 500 µL of the respective inoculum. The inoculum was uniformly spread all over the agar plate by using the lawn culture method. The culture plates were placed in the incubator for 24 hours at 37℃. After incubation, the plates were taken out of the incubator and the zones of bacterial inhibition were recorded in millimeters by using a digital caliper. Measurements were taken at the greatest distance between two points at the outer limit of the inhibition halo formed around the wells.13 This measurement using the digital caliper was repeated three times, and the mean was calculated for each well.
Assessment of fluoride release of glass ionomer cements
A fluoride release assessment was carried out at Maharashtra Public Health Engineering Department, District Public Health Laboratory, Dhule, Maharashtra, India. All the three GICs were tested to determine the amount of fluoride released into the de-ionized distilled water. Five specimens of each material were prepared. Immediately after mixing the cement, the materials were placed in a plastic mold measuring 4 × 4 mm. All specimens were made in the same mold to guarantee the same total surface area. After preparation, the specimens were placed in test tubes containing 50 mL of de-ionized distilled water and the fluoride ions released in the distilled water were assessed using calibrated a fluoride ion selective electrode (sensION Fluoride Ion Selective Electrode, HACH Company, Loveland, CO, USA) as per the manufacturer's instructions, after a period of 24 hours.
Statistical analysis
The data were analyzed using IBM SPSS Statistics for Windows Version 19 (IBM Corp., Armonk, NY, USA). The homogeneity of variance in each group was confirmed before analyzing the data. The mean values of the diameter of the zone of inhibition for the material in the three groups were analyzed. The mean inhibition zones of the materials against the two bacterial strains under consideration were compared for the three groups using analysis of variance (ANOVA). The post hoc Tukey highly significant difference (HSD) test was performed to identify the differences in the zone of inhibition for pairwise comparison. The difference in the amount of fluoride released for the three groups was tested using ANOVA followed by the post hoc Tukey HSD test. The significance level of the difference of the statistical test was set at 5%.
Results
It has been found that all the GICs considered in this study have antibacterial properties against S. mutans and L. acidophilus. D-tech showed the largest diameters of the zone of growth inhibition against both the strains (Table 1). Ketac Molar, on the other hand, presented the smallest zones of bacterial growth inhibition, probably resulting in a relatively low antibacterial power. A comparison using ANOVA showed a highly statistically significant difference (p < 0.001) in the mean diameters of the zone of inhibition for S. mutans and L. acidophilus among the three materials. In the pair-wise comparison using the post hoc Tukey HSD test, the difference in the mean diameter of the zone of inhibition for S. mutans between Fuji IX vs. Ketac Molar, Ketac Molar vs. d-tech, and Fuji IX vs. d-tech was found to be significant. The mean fluoride release was higher in the case of the d-tech cement than in the cases of Fuji IX and Ketac Molar (Table 2).
Discussion
This preliminary study determined the antibacterial effectiveness of different glass ionomers used in restorative dentistry by observing the zone of inhibition around the experimental samples in the culture plates. The present study was divided into two parts in order to evaluate the antimicrobial efficacy of three different GICs. The first part involved the evaluation of the antibacterial phenomenon of the three different GICs by using an agar diffusion microbiological assay procedure, and the second part consisted of an analysis of the fluoride release of the three different test cements by using an ion selective electrode.
In the present study, the Fuji IX and Ketac Molar GICs were selected as they are recommended for atraumatic restorative treatment. The d-tech GIC was selected because of its widespread usage, easy availability, economic feasibility, and a lack of scientific literature regarding its antimicrobial efficacy. Double blinding was achieved by keeping both the laboratory technician and the statistician blind. The laboratory technician was blind to the details of the plate and the cements, whereas the statistician was blind to the material groups while analyzing the data.
In the present study, the mean diameter of the bacterial inhibition zone for Fuji IX in the case of S. mutans was found to be 10.84 mm after an incubation period of 24 hours (Table 1). These results are in agreement with those of the study done by da Silva et al.12 and Luczaj-Cepowicz et al.14 The mean diameter of the inhibition zone for Ketac Molar in the case of S. mutans was found to be 10.23 mm after the 24 hours incubation period. These results are in accordance to the findings of da Silva et al.,12 wherein the zone of inhibition after 48 hours of incubation was found to be 10.00 mm. The mean diameter of the inhibition zone for the d-tech cement in the case of S. mutans was found to be 15.65 mm after the 24 hours incubation period. The results for the d-tech cement could not be compared with those of some other studies as, to the best of our knowledge, thus far, no previous research has been done to assess the antimicrobial efficacy of d-tech cement.
In the present study, in the comparison of the effect of Fuji IX on L. acidophilus, the mean diameter of the bacterial inhibition zone was found to be 10.4 mm after the 24 hours incubation period (Table 1). These results are inferior when compared with those of the study done by da Silva et al.,12 wherein the diameter of the bacterial inhibition zone after 48 hours of incubation was 11.8 mm. In the comparison of the effect of Ketac Molar on L. acidophilus, the mean zone of the bacterial inhibition was found to be 10.16 mm in diameter after the 24 hours incubation period. The zone of inhibition obtained in the present study is less than those observed in the study done by da Silva et al.,12 wherein the diameter of the bacterial inhibition zone after 48 hours of incubation was 12.6 mm. These inferior results might be attributed to the difference in the amount of inoculum used, the difference in size of the Petri dish used, and the different method of inoculation (lawn culture, which was used in the present study). The difference in the amount of inoculum may influence the zone of inhibition. A large amount of inoculum shortens the critical time and can result in a falsely smaller zone of inhibition, while a small amount of inoculum will cause the reverse effect and generate a falsely larger zone of inhibition.15 The mean zone of inhibition exhibited by d-tech cement in the case of L. acidophilus was found to be 15.57 mm after the 24 hours incubation period in the present study. The antimicrobial activity was in the sequence of d-tech > Fuji IX > Ketac Molar for both S. mutans and L. acidophilus.
In the present study, although all the cements were used in equal quantities and the same amount of inoculum was used, a statistically significant difference was observed in the antimicrobial activity of the three cements. This may be attributed to the fact that GICs are complex materials and no two commercial systems are chemically or mechanically identical.16 It is widely known that the inoculum size of the test organism considerably influences the size of the inhibition zones in the agar diffusion assay technique. A large amount of inoculum shortens the critical time and can result in a falsely smaller zone of inhibition, while a small amount of inoculum will cause the reverse effect and generate a falsely larger zone of inhibition.17 In the present study, the amount of inoculum used was 500 µL, whereas the amount of inoculum used in the study conducted by da Silva et al.12 was 300 µL. The difference observed between the present study and the other studies mentioned above may be attributed to the difference in the size of the Petri dish used and the different method of inoculation (lawn culture, which was used in the present study).
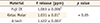
The antibacterial efficacy of cements has also been related to a low pH during initial setting, fluoride release, and other antimicrobial components present in the powder of these cements. GICs release various ions, of which fluoride has expressed antibacterial properties and presented the potential of preventing caries. Fluoride is considered to be one of the major elements responsible for the antimicrobial effect of these cements. Hence, we had to check the amount of fluoride released by these cements. A higher fluoride release was observed in the case of the d-tech cement than in the cases of the other two cements we considered (Table 2). The amount of fluoride release has been related to the composition and the setting reaction of the material. The high-strength conventional GICs Fuji IX and Ketac Molar present high powder/liquid ratios that improve their mechanical properties for the restoration of posterior teeth. However, this can result in decreased solubility and fluoride liberation.12 The d-tech cement has a lower powder/liquid ratio than the other two cements. This might be the reason for the increased antibacterial efficacy of the d-tech cement, and further research is required in this direction. The antibacterial efficacy of all the cements considered in the present study may also be attributed to the presence of other elements in the cements, such as zinc and strontium, but the present study did not assess these factors due to feasibility issues.
As mentioned above, in this study, other antimicrobial constituents of GICs, such as zinc and strontium, could not be assessed because of feasibility issues. The nature of the fluoride released, whether loosely or structurally bound, could also not be determined. Further studies should be conducted to understand the exact mechanism behind the antimicrobial activity of the d-tech cement. Moreover, the remineralization potential of the d-tech cement should be evaluated. Long-term clinical trials should also be carried out to assess the antibacterial efficacy of different GICs.
Conclusions
On the basis of the results of the present study, we can conclude that all the GICs we evaluated demonstrated antibacterial activity with differences according to the material. Furthermore, the d-tech cement showed the best antibacterial activity among the three cements tested, which could be an advantage in terms of its use in regular clinical practice.

 XML Download
XML Download