

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
An ideal root canal filling should fill the entire root canal system in three dimensions and form a homogenous mass.1 Warm vertical (WV) compaction of gutta-percha was proposed in the 1960s,1 and this technique has been shown to lead to satisfactory results in terms of homogeneity and to fill a high percentage of the root canal area with gutta-percha material.2 However, the armamentarium required for this technique is considerably more expensive than is required for cold lateral (CL) compaction. Another criticism of this thermoplasticized technique is that apical control of the filling material can be difficult at times, and some material may be extruded beyond the apical foramen.3
CL compaction of gutta-percha, also commonly known as the CL condensation technique, is probably the most commonly taught and utilized technique worldwide.4 It has often been used as a reference point for the evaluation of other obturation techniques. It is a less technique-sensitive method than WV compaction and has a lower start-up cost. However, cold gutta-percha cannot adapt well to canal irregularities, and a considerable amount of voids may be present between the gutta-percha cones and the root canal wall.5 Moreover, CL compaction is unable to effectively seal lateral canals.6 Studies have indicated that CL condensed gutta-percha cones remain separate, without merging into a single homogenous mass.7 The wedging force generated as gutta-percha points are compressed to create accessory cones may predispose the tooth to vertical root fracture, especially with overzealous compression.89
Ultrasonic devices are common equipment in modern dental offices. When operated dry, the frictional heat generated by an ultrasonic instrument can be used to plasticize the gutta-percha during obturation. The use of a size 25 K-file attached to a magnetostrictive ultrasonic unit to assist the placement of gutta-percha root filling was first described in the 1970s.10 Thereafter, studies have shown that obturation using ultrasonic energy produces a significantly denser and more homogenous root filling than is obtained by CL compaction.1112 In such studies, the final gutta-percha mass showed good adaptation to canal surface irregularities with fewer voids.13 With the exception of an extended period of intracanal activation at maximum power that may result in a significant rise in temperature,14 the temperature rise on the external root surface is generally within 10℃ at all levels of the root, which is safe for periodontal health.15 However, the ultrasonic compaction of gutta-percha has failed to become a popular method for root canal obturation, perhaps due to the emergence of various heating devices that can expedite the delivery of thermoplasticized gutta-percha into the root canal.
High-resolution computed tomography (micro-CT) has been used in endodontic research for more than a decade. Its high accuracy and ability to reveal fine details without destroying specimens make it a valuable tool for examining the internal structure of hard tissues or dental materials.16 Micro-CT has been used in the study of root canal anatomy,17 morphological changes in the root canal due to different instrumentation techniques,18 and to study obturation materials and techniques.192021 Micro-CT images have been compared with those from histological sections, confirming that micro-CT can accurately capture the three-dimensional (3D) morphology of root filling material.22
The purpose of the present study was to determine the quality of root canal fillings obturated with WV compaction, CL condensation, and ultrasonic lateral (UL) compaction. The quality of the fillings were evaluated by the volume fraction of the root canal space occupied by gutta-percha within the mesial canals of mandibular first molars, as determined using micro-CT imaging. The null hypothesis of the study was that these three techniques would not lead to statistically significant differences.
Materials and Methods
Permanent mandibular first molars were obtained from an extracted tooth bank and evaluated radiographically for the presence of separate mesiobuccal and mesiolingual canals in the mesial root. All teeth were examined under magnification to exclude those with root fillings, resorptive defects, cracks, root fractures, immature apices, root caries, or metallic restorations. Thirty-three teeth were finally selected.
Root canal preparation
After preparing an endodontic access cavity, the coronal part of each root canal was flared using Gates-Glidden drills. The working length was established 0.5 mm from the apical foramen by exploring with a small (size 10) K-file and examination under magnification. Root canals were negotiated and prepared manually with K-Flexofile files (Dentsply Maillefer, Ballaigues, Switzerland) to a size corresponding to size 20 files, then by ProFile rotary instruments (Dentsply Maillefer) to an apical size of corresponding to a size 30, 0.06 taper instrument. Patency was maintained using a size 10 K-file. Canals were irrigated with 3 mL of sodium hypochlorite after the use of each instrument with a 27-gauge side-exiting needle (Endodontic irrigation syringe with needle, Monoject, Covidien, Mansfield, MA, USA).
After canal preparation, a master gutta-percha cone was fitted into each canal such that a 'tug-back' sensation was felt. Radiographs were taken in both the buccolingual and mesiodistal planes. Root canal curvature was measured on both radiographs for every canal using Pruett's method.23 The specimens were then divided using stratified sampling, according to the canal length and curvature, into three groups for obturation using the CL, UL, or WV techniques.
In the stratified sampling process, the specimens were first divided into two major groups according to the canal's buccolingual curvature. Subgrouping was then carried out for each major group according to the mesiodistal curvature. Further stratification according to canal length was performed to produce the three final experimental groups. Specimens from each of these final groups were randomly allocated into an experimental group, with each group containing 11 teeth and a total of 22 canals. Normality tests and one-way analysis of variance were performed to confirm the comparability of the groups.
Obturation procedures
Prior to obturation, the canals were irrigated with 5 mL of 3% sodium hypochlorite and 5 mL of 17% ethylenediaminetetraacetic acid (EDTA). The canal was then dried with paper points. In order to prevent the masking of any voids within the gutta-percha material, root canal sealer was not used during the obturation process.
1. Cold lateral compaction (Group CL)
The procedures described in a textbook were followed. Briefly, a master gutta-percha cone (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) of the same size as the master apical file was chosen.24 It was adjusted until 'tug-back' was achieved and then seated to the working length. A finger spreader (size MF, SybronEndo, Orange, CA, USA) was inserted 2 - 3 mm from the working length. An accessory cone (Size FF, Dentsply Maillefer) was added and compressed with the finger spreader. This procedure was repeated until the spreader could no longer be inserted for more than 2 mm into the canal orifice. Excess gutta-percha was then removed with a hot instrument 0.5 mm below the orifice and compressed in the apical direction with a cold plugger.
2. Energized warm lateral compaction with ultrasonic spreader (Group UL)
A master gutta-percha cone was selected, adjusted until 'tug-back' was observed, seated to working length, and compressed with a finger spreader in the same manner as described above for the CL group. Two accessory cones (size FF) were then inserted and compressed with the finger spreader, followed by the use of a 0.02-taper, spreader-like, smooth-sided nickel-titanium instrument (ESI instrument; Electro Medical Systems SA, Nyon, Switzerland) activated at the lowest power setting using an ultrasonic machine (MiniMaster LED, Electro Medical Systems SA). This ultrasonic spreader was gradually sunk apically up to 2 - 3 mm from the working length. Another accessory cone was subsequently inserted, compressed with a cold spreader, and then compressed using the ultrasonically activated instrument. This process was repeated until the cold spreader could not be inserted for more than 2 mm into the canal orifice. Excess gutta-percha cones were seared 0.5 mm below the orifice and compressed with a cold plugger. The technique was similar to that described by Bailey et al.1314
3. Warm vertical compaction (Group WV)
This obturation technique requires the use of non-standard tapered cones.25 For this group, size FM gutta-percha cones (Dentsply Maillefer) with the tip adjusted to correspond to the size of the apical terminus were used as the master cone. A short, crisp 'tug-back' sensation was felt.25 A heating device (Touch'n Heat Model 5004, Analytic Technology, Redmond, WA, USA) was used to sear off and soften the gutta-percha near the root canal orifice. The gutta-percha was then compressed vertically (in the apical direction) using a cold Machtou plugger (Dentsply Maillefer). Heat was applied again with the heating device placed more deeply (approximately 2 - 3 mm) in the canal, followed by the use of a smaller plugger. The process was repeated until 4 - 5 mm of gutta-percha remained in the apical portion of the canal. The middle and coronal thirds of the canal were then filled by an injectable thermoplasticized gutta-percha system (Obtura II, Obtura-Spartan, Algonquin, IL, USA) up to 0.5 mm below the canal orifice, followed by compression with a cold plugger.
Micro-CT analysis
Each tooth was mounted on a custom-made holding device for imaging in a micro-CT scanner (Skyscan 1172, Bruker-microCT, Kontich, Belgium) operating at 100 kV, 100 mA, 360° rotation, 1.5° rotation steps, and 7.9-µm voxel size. Imaging was performed both before and after the obturation procedure. The resultant images were rendered in a proprietary software (NRecon version 1.6.6, Bruker-microCT) to obtain 3D pre- and post-obturation records of each specimen. The 3D images were imported into MeVisLab version 2.5 (MeVis Medical Solution SA, Bremen, Germany) for volume measurement. Each canal was arbitrarily divided into 2 mm segments beginning from the apical terminus of the root filling, and the volume fraction of gutta-percha present within the prepared canal space in each segment was calculated using the MeVisLab software.
Statistical analysis
The overall mean fraction of the root canal volume filled with gutta-percha for each group was determined, as well as the 95% confidence interval. The results for each group were compared using SPSS version 20.0 for Windows (IBM Corp., Armonk, NY, USA) with a significance level of p < 0.05. The effects of the obturation method and distance from the apical terminus on the volume fraction were examined using two-way analysis of covariance (ANCOVA), followed by post-hoc pairwise comparisons with the Bonferroni correction in order to evaluate the impact of obturation technique and root canal level.
Results
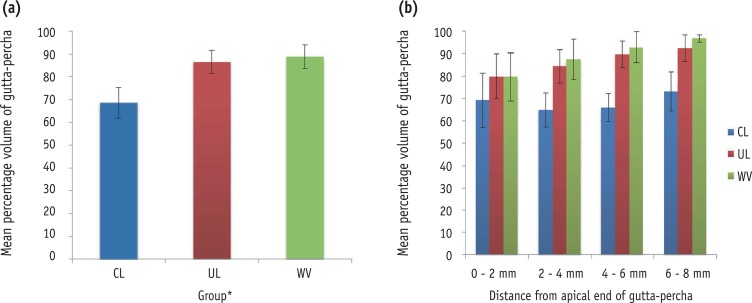
Statistically significant differences were noted in the overall amount of gutta-percha within the root canals obturated using these three techniques (Figure 1a). The overall gutta-percha volume was significantly lower in the CL group than in the UL and WV groups (p < 0.05). Two-way ANCOVA indicated that the location of the root segment and the obturation technique had a significant impact on the quality of obturation.
Effect of the obturation method
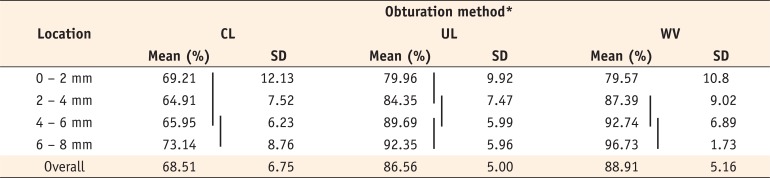
When root segments at the same level or distance from the apical foramen were compared among the groups, the mean volume fraction of the root canal space occupied by gutta-percha was significantly lower in the CL group than in the UL or WV groups (p < 0.001 for both CL vs. UL and CL vs. WV). No significant differences were observed between the UL and WV groups at similar locations along the root (p = 0.526, Figure 1b).
Micro-CT appearance
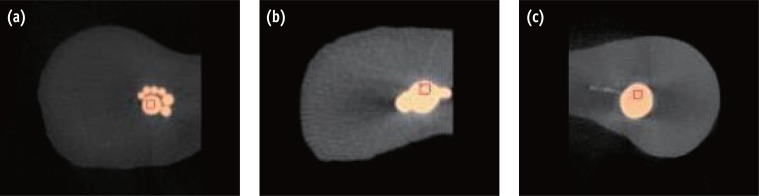
In the roots treated with cold lateral compaction, minimal distortion of the gutta-percha cones was observed, that is, the outline of individual cones could be seen on the micro-CT images (Figure 2a). The gutta-percha in the CL group did not extend into the recesses and was not in close contact with the root canal wall. In the apical 2 mm of the canal, only a single gutta-percha cone was noted in the majority of the roots (19 out of 22 canals). In the UL (Figure 2b) and WV groups (Figure 2c), the outline of individual cones often became indistinguishable, since the gutta-percha became a homogenous mass that adapted to the irregularities along the root canal. In these canals, voids were very occasionally detected between the apical part ('downpack') of the root filling and the injectable gutta-percha.
Discussion
A limited amount of studies have evaluated the application of ultrasonic energy to facilitate root canal obturation. Some authors have examined the induced temperature rise,1415 the density of the root filling,12 the sealing ability,1113 and the surface topography of the root filling.11 However, no study has attempted to volumetrically quantify the extent of root canal filling achieved through ultrasonic obturation. As in any study involving extracted teeth, it was not possible to completely standardize the internal root canal anatomy, especially in cross-sections. We attempted to standardize the longitudinal configuration as much as possible, both with regard to canal length and curvature. An ideal technique would have enabled the gutta-percha cones to fill the canal space in three dimensions, regardless of the cross-sectional morphology.
Clinically, root canal sealer is used during root canal obturation to help fill irregularities and gaps. The sealer can penetrate into dentinal tubules and may serve as a lubricant that facilitates insertion of the gutta-percha cones. It is possible that applying a sealer might enhance the volume fraction of gutta-percha in the canal after obturation to some extent. However, sealers are often radiopaque, and the use of a sealer in this study would have added another independent variable to this study, as different sealers may have different rheological properties, and would have been likely to affect the micro-CT detection of voids within the bulk of the root filling. A similar protocol, in which sealer is not used, has been employed in other studies.131426 It has been pointed out that the radiographic borders between dentine, sealer, and gutta-percha are difficult to distinguish when a root canal sealer is used.22 Therefore, a root canal sealer was purposefully omitted in this study to improve the detection of the dentine-gutta-percha interface.
The CL compaction technique resulted in minimal distortion of the gutta-percha cones, and the outlines of individual cones could often be seen on the micro-CT images. The cold gutta-percha did not extend into the recesses of the canal and was not in close contact with the root canal wall. Similar observations have also been reported in other studies.727 In the apical 2 mm of the canal, often only a single gutta-percha cone was present, and that the master cone was in contact with only part of the entire canal wall, but not the entire perimeter. This finding corroborated those of Wu et al.28 In more coronal areas, many of the gutta-percha cones remained separate and discrete, with noticeable space present among individual cones. Likewise, similar observation has been reported previously.29 The aggregate of these observations indicate that CL compacted gutta-percha cones are less than ideally adaptable, both to the root canal wall and to one another.
The protocol for UL compaction have varied among studies. In particular, no consensus exists regarding the power setting for the ultrasonic generator. The recommended setting has been left to individual preference, which may lead to variation in the results that have been reported. In our study, we began with the lowest power setting and observed that the spreader advanced gradually to the desired length in five to 10 seconds, which we considered reasonable. Little tactile sensation was lost and satisfactory control of the spreader could be maintained. For this reason, that power setting was adopted. During the process, two accessory cones were inserted after the master cone and before the application of the ultrasonic spreader. This was done to avoid direct contact of the spreader with the root canal wall, to avoid scoring the dentine, and to ensure complete transmission of energy to the gutta-percha mass. Once resistance to apical advancement was felt, the ultrasonic spreader was withdrawn, and a finger spreader was then used. With this method, the coronal part of the gutta-percha filling was effectively plasticized, thereby allowing deeper penetration of the spreader. An increase in the density of gutta-percha, especially towards the coronal aspect, was expected. The density of the gutta-percha filling at the apical region was also greater when an ultrasonic spreader was used than when CL compaction was used, indicating that UL compaction led to an overall improvement of the obturation quality. The extent of plasticization of the gutta-percha cones was revealed by micro-CT evaluation. The density of the resultant filling was on par with that achieved by WV compaction of gutta-percha. Hence, for those practitioners who are accustomed to using the lateral compaction technique, or who would not wish to invest in the equipment necessary to perform the WV compaction technique, UL compaction may be a useful alternative.
The gutta-percha-filled volume obtained by WV compaction was similar to that obtained using UL compaction. Micro-CT images revealed the presence of gaps between the canal wall and the master cone in some sections. This observation was likewise reported by Wu et al., who noted that the most apical part of the root canal was often incompletely filled when the WV compaction technique was used.26 Some authors have suggested that such gaps may be caused by insufficient heating of gutta-percha within the canal.27 The injectable gutta-percha that fills the middle and coronal third of the canal (after the 'downpack') provided a homogenous mass with minimal voids in the coronal segments.
In light of the differences in the volume fraction of gutta-percha among the three techniques that we examined, the null hypothesis was rejected. Thermoplasticized techniques are able to mediate a closer adaptation of gutta-percha to the root canal wall than CL compaction, and the improved obturation quality did not depend on the cross-sectional shape of the root. However, none of the obturation techniques tested in this study were able to express any gutta-percha into any lateral canals, or to fill the isthmus entirely. Thus, the use of a root canal sealer is required during root canal obturation in the clinical context. Root canal sealer would also fill the voids within the root canal system that were noted in the micro-CT images in this study. Root canal sealer is therefore essential for any obturation technique involving gutta-percha, including thermoplasticized techniques.
The results of this study demonstrated the promise of using the UL compaction technique to help plasticize the gutta-percha in root canal. This technique is likely to involve a low start-up cost, as most dental practices already have ultrasonic equipment. It is also easy to learn, as it is based on CL compaction, which is commonly taught. It is true that ultrasonic spreading does not speed up the obturation process in comparison with CL compaction, but it improves the quality of the gutta-percha filling. Furthermore, the ESI instrument, which is a smooth conical spreader-like instrument, is able to prevent the inadvertent cutting of dentine during the energized compaction process. Lateral compaction of gutta-percha with an ultrasonic spreader is an effective alternative to, and requires a lower start-up cost than, WV compaction. Higher quality root canal fillings are likely to result from the implementation of ultrasonic spreading in place of the CL compaction technique.


 XML Download
XML Download