

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Translucency in esthetic restorative materials induces the depth of color in restorations, and also influences the color harmonization with surrounding or adjacent teeth/restorations.123 Optical performance of restorations may be compromised by poor shade blending of opaque restorative materials at the tooth interface.4 For the measurements of optical properties, the Commission Internationale de I'Eclairage (CIE) color coordinates and the CIE standard illuminants are generally used.5 For the determination of translucency, two indices such as translucency parameter (TP) and contrast ratio (CR) have been widely used.67 TP is obtained by calculating the color difference of a specimen over two backgrounds: TP = [(LW* - LB*)2 + (aW* - aB*)2+ (bW* - bB*)2]1/2, where subscript W refers to the color coordinates over an ideal white background and subscript B refers to those over an ideal black background.6 CR is calculated from the spectral reflectance (Y) of the specimens over black (Yb) and white (Yw) backgrounds to give Yb/Yw.7 Mean CR is calculated as the averaged CR values at each wavelength (10 nm intervals) in the range of 400 to 700 nm.89 Since it has been confirmed that TP and CR values are highly correlated,89 they might be used interchangeably.
Care must be taken when comparing the translucency values based on different studies because technical details for measurements must be matched, or adjustments must be made.10 Therefore, for the evaluation of translucency based on reported values, the followings should be checked thoroughly: (1) Measuring instrument and method should be specified because both of them influence the values.9 Reflection spectrophotometer with an integrating sphere could be regarded as a reference instrument; (2) Thickness of specimen influences the translucency values.911 Regression equations that can reflect the influence of the thickness on the translucency values might be established.9 However, these equations would be influenced by the measurement methods; (3) Optical properties of backgrounds used for translucency measurement should be specified.12 As reference values for ideal backgrounds, the CIE color coordinates of background were reported as CIE L* = 94.3, a* = -0.4, and b* = 1.4 for the white background, CIE L* = 0.2, a* = 0.4, and b* = -0.6 for the black background and CIE L* = 0.0, a* = 0.0, and b* = 0.0 for a zero calibration box in a previous study.12 The translucency values may also be modified which would reflect the color difference of the two backgrounds such as TPcomparative = color difference of a specimen over white and black backgrounds/color difference of white and black backgrounds themselves; (4) Illuminating conditions influence the translucency values.1314 Generally used illuminant such as the CIE illuminant D65 could be regarded as a reference illuminant.
In a previous review on the translucency of dental substances,3 the following subjects such as translucency of teeth, clinical relevance of translucency, measuring methods, and the control of translucency in esthetic materials were reviewed. The purpose of the present review was to suggest criteria for the clinical translucency evaluation, and to review the translucency of direct esthetic restorative materials based on translucency of human enamel and the visual perceptibility threshold for the translucency difference. For this, PubMed search up to 2015 was carried out for papers on the translucency of direct esthetic restorative materials published in English. Additional articles were searched by hand-searching based on the references of the included papers. Search results from other major databases were overlapping to those from PubMed and hand-searching. As to the statistical significance of the results in the present article, it was regarded as significant if the p value was lower than 0.05.
Review
Criteria for translucency evaluation
The criteria for the clinical evaluation of translucency were established from two aspects: (1) whether the values are similar to those of human enamel, or (2) whether the differences between the compared materials are perceivable by the naked eyes.
1. Translucency of human teeth
Translucency of human teeth should be the reference in the translucency assessment of esthetic restorative materials.3 As to the translucency of intact teeth, translucency differences in human maxillary central incisors by anatomic locations were analyzed, and was reported that the transmission ranged from 0.13 to 0.65%, which decreased from incisal to cervical area.15 Translucency of human central incisors was measured using a spectroradiometer,16 and the color difference over white and black cloths behind the intraoral teeth was reported as TP. As results, translucency decreased from the incisal to cervical, where TP of incisal site was approximately 15, which decreased to around 5 at cervical site. However, these values were based on whole teeth, whereas restorations are usually built up by layering technique.
As to the translucency of separated enamel and dentin, it was reported that the light transmission of human enamel increased as the incident light wavelength increased.17 Translucency of human and bovine enamel/dentin was determined by use of TP and CR.9 In this study, two spectrophotometers with different aperture sizes of 3 mm round (TP3) and 3 × 8 mm rectangular aperture (TP38) were used. As results, mean TP3 values of 1 mm thick bovine enamel, bovine dentin, human enamel and human dentin were 14.7, 15.2, 18.7, and 16.4, respectively. It was also confirmed that the translucency of enamel and dentin increased in proportion to wavelength in the visible range (correlation coefficient: r = 0.87 - 0.91).9
In addition to the translucency value itself, optical anisotropy of teeth should be another consideration. Translucency of an object is estimated in a consistent way across different shapes and lighting conditions to some extent (translucency constancy). However, humans also show significant failures of translucency constancy across changes in lighting direction.18 Transmitted light intensities in the direction perpendicular or parallel to the approximal surface of tooth were compared to account for a directional dependence of light fluxes.19 The results indicated that the mean ratio of the transmitted intensities in perpendicular and parallel direction was 0.86 for enamel and 2.88 for dentin.
2. Visual perceptibility threshold of translucency
Relationship between a translucency index (CR) and the subjective visual assessment of differences in the translucency of dental porcelains with different opacities was determined.20 Translucency range of group A (CR = 0.20 to 0.40) was equivalent to that of enamel porcelain, whereas group B (CR = 0.60 to 0.80) represented dentin porcelain translucency based on 1 mm thick specimens. Each observer's ability to distinguish between specimens of different translucencies was determined by calculating the mean perceivable minimal difference in CR (ΔCR), which was named as 'translucency perception threshold (TPT)'. As results, when pooling the data for two light conditions (transmitted and reflected lights) and two porcelain types, mean ΔCR of three observer groups was 0.09 for students, 0.08 for residents, and 0.04 for faculty. The overall mean TPT of all observers was 0.07. In high translucent group (CR = 0.20 to 0.40), mean TPT was lower than that of low translucent group (CR = 0.60 to 0.80) under both lights. Therefore, translucency difference in CR (ΔCR) of 0.07 was regarded as the perceivable limit, which could be suggested as the second criterion of the present review. Since this value was determined based on CR,20 the need for an establishment of correlation between the translucency indices was raised for the application of this value to another index (TP).
3. Correlation between translucency indices
Since translucency values varied by the measurement protocols, correlations among them should be confirmed. Correlations among the translucency values based on different measurement methods were reviewed in this section.
TP and light transmittance (%T) were positively correlated (r = 0.63) based on 1 mm thick resin composites.21 CR increased in inverse proportion to TP (r = -0.93) based on resin composites and an all-ceramic material with the thickness of 0.8, 1.3, and 1.8 mm.22 Based on varied shades and brands of resin composites, the correlation between TP and CR was determined based on 1 mm thick specimens.8 As results, a regression equation 'TP = -28.2 × (mean CR value) + 32.8' was obtained (r = -0.84). Applying this equation, threshold ΔCR value for TPT of 0.0720 could be transformed into ΔTP value of 2 when TP values were around those of human enamel (TP = 15 to 19).
TP and CR of human and bovine enamel/dentin were determined.9 Mean CR values of human and bovine enamel/dentin were negatively correlated with TP (r = -0.93 to -0.78) based on a spectrophotometric readings with 3 mm round aperture (TP3). Regression equations between TP3 and mean CR of human enamel and dentin were TP3 = -36.3 × (mean CR) + 38.9 (coefficient of determination: r2 = 0.83) and TP3 = -22.9 × (mean CR) + 29.2 (r2 = 0.62), respectively.
Based on TP values of human and bovine enamel/dentin,9 correlations in these values by the measurement methods were also reported. Two spectrophotometers with different aperture sizes of 3 mm round aperture (TP3) or 3 × 8 mm rectangular aperture (TP38) were used. The results showed significant correlations between TP values measured with two apertures. Mean TP3/TP38 values of 1 mm thick bovine enamel, bovine dentin, and human dentin were 14.7/18.3, 15.2/21.1, and16.4/21.7, respectively (r = 0.87 - 0.98). Regression equation between TP values of human dentin were TP38 = 1.0 × TP3 + 5.1 (r2 = 0.77). As to the influence of thickness, ranges of thickness in bovine enamel, bovine dentin, human enamel, and human dentin specimens were 0.9 - 1.3, 1.0 - 2.0, 0.9 - 1.6, and 0.7 - 1.6 mm, respectively. TP values increased in inverse proportion to the thickness (r = 0.80 - 0.90). Regression equations between TP of human enamel/dentin and the thickness (mm) of specimens were TP3 = -12.7 × thickness + 31.4 (r2 = 0.64) and TP3 = -9.3 × thickness + 25.7 (r2 = 0.71), respectively.
Range of translucency in direct esthetic materials
1. Translucency variations by type or shade of resin composites
There have been studies that compared the translucency of resin composites. Comparisons were made by (1) the type of resin composites, (2) shade groups such as dentin, enamel, translucent, incisal and opaque shades, and/or (3) brand of composites. Translucency of resin composites was also compared with other kinds of direct esthetic materials.
1) Difference by type of resin composites
Translucency differences between direct/indirect, universal/flowable, or other types of resin composites were determined. As to the translucency differences between direct and indirect resin composites, translucency of indirect (BelleGlass NG, BG, Kerr, Orange, CA, USA) and direct (Estelite Sigma, ES, Tokuyama, Tokyo, Japan) resin composites, each composed of three shade groups, was compared based on 1 mm thick specimens.23 As results, mean TP after curing were in the range of 10.0 (BG-opaceous dentin shade) to 21.5 (BG-enamel shade) (Figure 1). BG material showed a wider range of TP values than ES. Therefore, translucency variations should be considered when an indirect resin composite restoration is repaired with direct composites. Since the differences in TP by the material and shade group combination were higher than 2, the differences were perceivable.
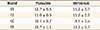
Translucency of flowable resin composites was compared with the corresponding shade universal composites of the same brand based on 2 mm thick specimens.24 As results, flowable composites revealed higher TP values in three of four brands (Table 1), and color difference between flowable and the corresponding universal resin composites was influenced by their translucency difference. Therefore, translucency differences between two types of composites should be reconsidered when two composites are used at the same. However, the differences in TP were not perceivable in three brands (ΔTP < 2).
TP values of flowable bulk-filling resin composites at various thicknesses (1 to 6 mm) were evaluated.1125 This type of composites can be filled in bulk up to 4 mm, which is used basically for primary teeth. Bulk-filling composites and conventional flowable/universal composites were investigated. As results, TP values were significantly correlated with the thickness of specimens. In bulk-filling composites, translucency was observed for thicknesses up to 5 to 6 mm, whereas it was observed up to 2 to 3 mm in flowable/universal composites. Therefore, bulk-filling composites showed less masking ability than the conventional composites. Translucency of composite framework materials was also determined.26 As results, glass-fiber-reinforced framework materials were nearly as translucent as the veneering dentin composite. However, these materials affected the color of the prosthesis if the thickness of the framework material was increased beyond a certain point (0.5 mm).
2) Difference by shade group
As to the translucency difference by the shade group and/or brand, translucency of seven brands of resin composites with three shade groups (dentin, enamel, and translucent) were compared based on TP and light transmittance (%T).21 As results, TP differed significantly by the brand within each shade group, and by the shade group within each brand. The results also showed strong correlation in translucency within each brand of resin composites except one brand (r = 0.76 - 0.99), and moderate correlation within each shade group (r = 0.40 - 0.53).
TP of resin composites at various thicknesses (0.5, 1, 2, 3, and 4 mm) was evaluated by the shade group of enamel, opaque, and body shades.27 In this study, black (CIE L* = 29.4, a* = -0.9, and b* = 0.1) and white (L* = 93.6, a* = -2.0, and b* = 3.5) backgrounds were used. The results indicated that the opaque shades were less translucent than the other shades, and that translucency increased exponentially as thickness was reduced regardless of the shade group. TP values of 1 mm thick specimens were 6.1 to 12.3 in one brand, and 7.4 to 13.1 in the other brand. TP values of 1 mm thick specimens were lower than those of human enamel (TP = 15 to 19) probably because the backgrounds used were not ideal black or white color.
TP and masking efficiency of opaque shade resin composites were determined.28 As results, opaque shade composites were less translucent than usual shade composites. Therefore, opaque shade composites might effectively mask the dark background color. Translucency of opaque shade (OA2) and conventional shade (A2) resin composites were evaluated based on 2 mm thick specimens.29 As results, TP values of OA2 were smaller than those of A2 for all the products investigated. TP values were 3.6 to 5.1 in A2 shade and 1.7 to 4.9 in OA2 shade, and the difference by the brand was significant. Adequate thickness range of opaque shade resin composites for masking the black oral cavity and discolored tooth structure was determined within the thickness range of 0.5 to 4 mm by 0.5 mm interval.30 Six opaque shade resin composites were investigated, and four backgrounds such as white tile, black tile, Vita C4 shade porcelain and opaque resin itself were used to determine TP, and to mimic a black oral cavity and a discolored tooth structure. As results, TP decreased in similar pattern as thickness increased. C4 background was masked with opaque resin thicknesses of 0.5 to 1 mm, while the black background required thicknesses of 1 to 2 mm.
2. Sorting of translucency in resin composites
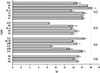
A wide range of translucency values indicates the need for establishment of reference points in sorting these values.31 TP of eight brands of resin composites (total 41 shades) were sorted based on 1 mm thick specimens (Figure 2 and Table 2).8 Since TP varied from 8.5 to 20.6, they were arbitrary divided into three groups at the TP values of 13 and 18 (Figure 2). Since the difference in TP between two reference values was 5, translucency difference between resin composites belonging to different groups was perceivable (ΔTP > 2). In this previous study published in 2008,8 no definitive clinical implication could be stated since there were no established criteria on the proper or acceptable translucency for esthetic restorative materials at that time. Instead, tentative sorting was made by dividing the TP values into three groups. According to TP value distribution of the study and because most of the investigated composites showed TP values within 13.0 to 18.0, translucency values were sorted into low, medium, and high groups. However, it should be remembered that the sorting was arbitrary for convenience.
Dividing translucency of resin composites into three equal segments was another solution.31 Therefore, TP of microhybrid (MH) and microfill (MF) resin composites were divided into three equal parts representing low, medium, and high translucency based on 2 mm thick specimens. As results, 15 shades of MH and 6 shades of MF were found to be of low translucency (TP = 0.9 - 2.0), 5 shades of MH and 1 shade of MF were of medium translucency (TP = 2.1 - 3.1), and 6 shades of MH and no MF shades were highly translucent (TP = 3.2 - 4.3). Since the color of black (CIE L* = 24.5, a* = -0.01, and b* = -0.4) and white (L* = 66.3, a* = -1.3, and b* = -4.0) backgrounds used in this study was far from ideal, TP values were relatively low.
3. Glass ionomer based materials
As to the translucency of glass ionomer based materials, opacity of glass ionomers were compared with that of resin composites.32 In 1983, newer glass ionomers were found to be more translucent than the first generation of glass ionomers. However, the opacity still needed to be reduced to reach the level of resin composite. With resin modified glass ionomers,33 translucency values varied according to whether the material had been subjected to light curing or cured through the acid-base reaction alone. As results, light cured specimens were found to be only marginally more translucent than those allowed to set without irradiation. Changes in the translucency of experimental 10 to 50% 2-hydroxyethyl methacrylate (HEMA)-added glass ionomers after 5,000 cycles of thermocycling were determined.34 As results, changes in TP were in the range of -3.5 to 0.2, and were influenced by the HEMA content and powder shade.
Conclusions
The criteria for the clinical evaluation of translucency were established from two aspects: (1) whether the values are similar to those of human enamel, and (2) whether the differences between the compared pairs are perceivable by the naked eyes. TP from 15 to 19 could be regarded as the value of 1 mm thick human enamel. Translucency difference in contrast ratio (ΔCR) of 0.07 was regarded as the perceivable limit, which could be transformed into ΔTP value of 2.
Comparisons of translucency were made by the type of resin composites such as direct/indirect or universal/flowable composites, and by the shade groups such as dentin, enamel, translucent, incisal and opaque shades. As to the difference between direct and indirect composites, the differences in TP values by the material and shade group were higher than 2. As to the difference between universal and flowable composites of the same brand and shade, the differences in TP values were lower than 2 in most brands. As to the difference by the shade group, TP value differed significantly by the brand within each shade group, and by the shade group within each brand. A wide range of TP values indicated the need for establishment of reference values for the interpretation of the values. Therefore, translucency of resin composites was categorized at the TP value of 13 and 18 as low, medium, and high translucency (1 mm thick), or divided into three equal segments.
The criteria proposed in the present article and the results of translucency evaluations could be used as guidelines for the clinical evaluation of translucency in direct esthetic restorative materials.


 XML Download
XML Download